Köhrle Josef, Lehmphul Ina, Pietzner Maik, Renko Kostja, Rijntjes Eddy, Richards Keith, Anselmo João, Danielsen Mark, Jonklaas Jacqueline
Institut für Experimentelle Endokrinologie, Charité Campus Virchow-Klinikum, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany.
Institute of Clinical Chemistry and Laboratory Medicine, University Medicine Greifswald, Greifswald, Germany.
Front Endocrinol (Lausanne). 2020 Jan 8;10:787. doi: 10.3389/fendo.2019.00787. eCollection 2019.
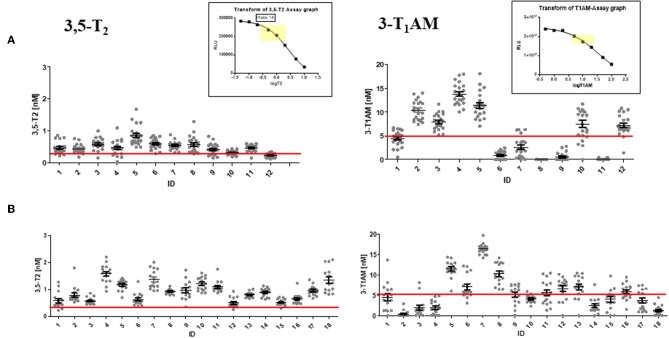
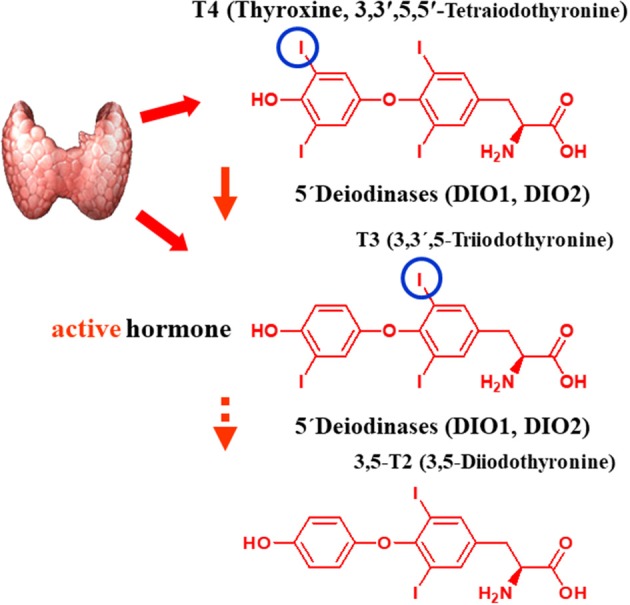
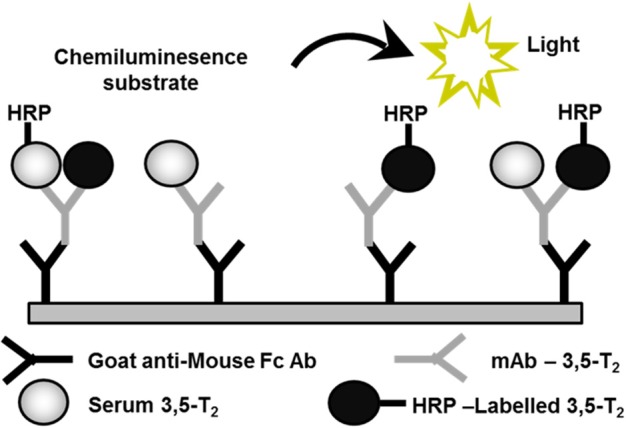
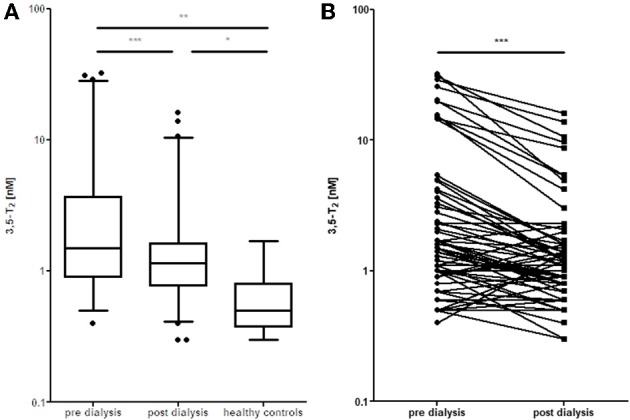
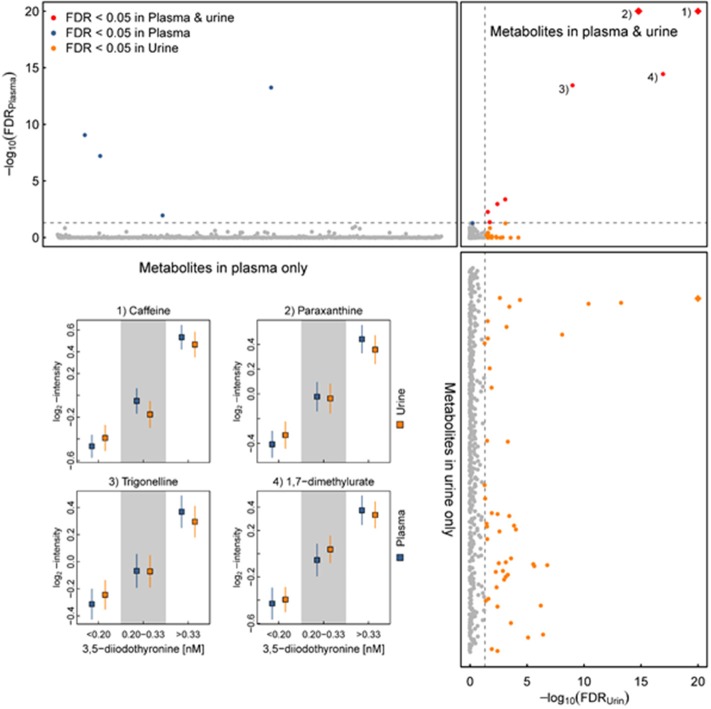
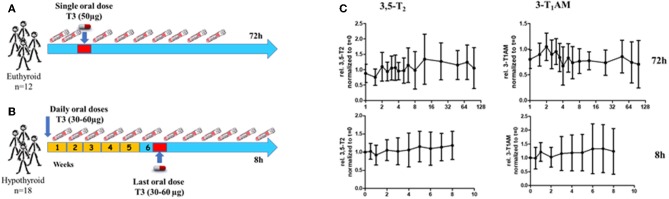
Over the last decades, thyroid hormone metabolites (THMs) received marked attention as it has been demonstrated that they are bioactive compounds. Their concentrations were determined by immunoassay or mass-spectrometry methods. Among those metabolites, 3,5-diiodothyronine (3,5-T2), occurs at low nanomolar concentrations in human serum, but might reach tissue concentrations similar to those of T4 and T3, at least based on data from rodent models. However, the immunoassay-based measurements in human sera revealed remarkable variations depending on antibodies used in the assays and thus need to be interpreted with caution. In clinical experimental approaches in euthyroid volunteers and hypothyroid patients using the immunoassay as the analytical tool no evidence of formation of 3,5-T2 from its putative precursors T4 or T3 was found, nor was any support found for the assumption that 3,5-T2 might represent a direct precursor for serum 3-T1-AM generated by combined deiodination and decarboxylation from 3,5-T2, as previously documented for mouse intestinal mucosa. We hypothesized that lowered endogenous production of 3,5-T2 in patients requiring T4 replacement therapy after thyroidectomy or for treatment of autoimmune thyroid disease, compared to production of 3,5-T2 in individuals with intact thyroid glands might contribute to the discontent seen in a subset of patients with this therapeutic regimen. So far, our observations do not support this assumption. However, the unexpected association between high serum 3,5-T2 and elevated urinary concentrations of metabolites related to coffee consumption requires further studies for an explanation. Elevated 3,5-T2 serum concentrations were found in several situations including impaired renal function, chronic dialysis, sepsis, non-survival in the ICU as well as post-operative atrial fibrillation (POAF) in studies using a monoclonal antibody-based chemoluminescence immunoassay. Pilot analysis of human sera using LC-linear-ion-trap-mass-spectrometry yielded 3,5-T2 concentrations below the limit of quantification in the majority of cases, thus the divergent results of both methods need to be reconciliated by further studies. Although positive anti-steatotic effects have been observed in rodent models, use of 3,5-T2 as a muscle anabolic, slimming or fitness drug, easily obtained without medical prescription, must be advised against, considering its potency in suppressing the HPT axis and causing adverse cardiac side effects. 3,5-T2 escapes regular detection by commercially available clinical routine assays used for thyroid function tests, which may be seriously disrupted in individuals self-administering 3,5-T2 obtained over-the counter or from other sources.
在过去几十年中,甲状腺激素代谢物(THMs)受到了显著关注,因为已证明它们是生物活性化合物。其浓度通过免疫测定法或质谱法测定。在这些代谢物中,3,5-二碘甲状腺原氨酸(3,5-T2)在人血清中的浓度为低纳摩尔水平,但至少根据啮齿动物模型的数据,其在组织中的浓度可能与T4和T3相似。然而,基于免疫测定法对人血清的测量结果显示,根据测定中使用的抗体不同,结果存在显著差异,因此需要谨慎解读。在甲状腺功能正常的志愿者和甲状腺功能减退患者的临床实验方法中,以免疫测定法作为分析工具,未发现3,5-T2由其假定前体T4或T3形成的证据,也没有找到支持3,5-T2可能是通过3,5-T2的联合脱碘和脱羧作用生成血清3-T1-AM的直接前体这一假设的证据,此前在小鼠肠黏膜中已有相关记录。我们推测,与甲状腺功能正常的个体相比,甲状腺切除术后或自身免疫性甲状腺疾病患者接受T4替代治疗时,3,5-T2的内源性产生降低,可能是导致部分接受该治疗方案的患者不满的原因。到目前为止,我们的观察结果不支持这一假设。然而,高血清3,5-T2与与咖啡摄入相关的代谢物尿浓度升高之间的意外关联需要进一步研究以作出解释。在使用基于单克隆抗体的化学发光免疫测定法的研究中,在包括肾功能受损、慢性透析、败血症、重症监护病房(ICU)非存活以及术后房颤(POAF)等几种情况下,均发现血清3,5-T2浓度升高。使用液相色谱-线性离子阱-质谱法对人血清进行初步分析,在大多数情况下,3,5-T2浓度低于定量限,因此两种方法的不同结果需要通过进一步研究来协调。尽管在啮齿动物模型中观察到了3,5-T2的积极抗脂肪变性作用,但考虑到其对下丘脑-垂体-甲状腺轴(HPT轴)的抑制作用以及导致心脏不良反应的可能性,必须建议不要将3,5-T2用作肌肉合成代谢、减肥或健身药物,因为它无需医生处方即可轻易获得。3,5-T2无法通过用于甲状腺功能测试的市售临床常规检测方法被常规检测到,在自行服用从非处方渠道或其他来源获得的3,5-T2的个体中,甲状腺功能测试可能会受到严重干扰。