Medicine Section, Veterans Affairs Salt Lake City Health Care System, Salt Lake City, Utah; and.
Department of Internal Medicine, University of Utah Health, Salt Lake City, Utah.
Clin J Am Soc Nephrol. 2020 Feb 7;15(2):200-208. doi: 10.2215/CJN.06600619. Epub 2020 Jan 23.
In early-phase studies of individuals with hypertensive CKD and normal serum total CO, sodium bicarbonate reduced urinary TGF-1 levels and preserved kidney function. The effect of sodium bicarbonate on kidney fibrosis and injury markers in individuals with diabetic kidney disease and normal serum total CO is unknown.
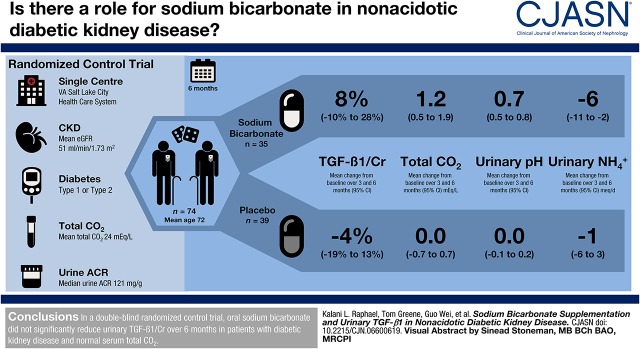
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We conducted a randomized, double-blinded, placebo-controlled study in 74 United States veterans with type 1 or 2 diabetes mellitus, eGFR of 15-89 ml/min per 1.73 m, urinary albumin-to-creatinine ratio (UACR) ≥30 mg/g, and serum total CO of 22-28 meq/L. Participants received oral sodium bicarbonate (0.5 meq/kg lean body wt per day; =35) or placebo (=39) for 6 months. The primary outcome was change in urinary TGF-1-to-creatinine from baseline to months 3 and 6. Secondary outcomes included changes in urinary kidney injury molecule-1 (KIM-1)-to-creatinine, fibronectin-to-creatinine, neutrophil gelatinase-associated lipocalin (NGAL)-to-creatinine, and UACR from baseline to months 3 and 6.
Key baseline characteristics were age 72±8 years, eGFR of 51±18 ml/min per 1.73 m, and serum total CO of 24±2 meq/L. Sodium bicarbonate treatment increased mean total CO by 1.2 (95% confidence interval [95% CI], 0.3 to 2.1) meq/L, increased urinary pH by 0.6 (95% CI, 0.5 to 0.8), and decreased urinary ammonium excretion by 5 (95% CI, 0 to 11) meq/d and urinary titratable acid excretion by 11 (95% CI, 5 to 18) meq/d. Sodium bicarbonate did not significantly change urinary TGF-1/creatinine (difference in change, 13%, 95% CI, -10% to 40%; change within the sodium bicarbonate group, 8%, 95% CI, -10% to 28%; change within the placebo group, -4%, 95% CI, -19% to 13%). Similarly, no significant effect on KIM-1-to-creatinine (difference in change, -10%, 95% CI, -38% to 31%), fibronectin-to-creatinine (8%, 95% CI, -15% to 37%), NGAL-to-creatinine (-33%, 95% CI, -56% to 4%), or UACR (1%, 95% CI, -25% to 36%) was observed.
In nonacidotic diabetic kidney disease, sodium bicarbonate did not significantly reduce urinary TGF-1, KIM-1, fibronectin, NGAL, or UACR over 6 months.
在高血压慢性肾脏病(CKD)患者和正常血清总 CO 的早期研究中,碳酸氢钠降低了尿转化生长因子-1(TGF-1)水平并保护了肾功能。在血清总 CO 正常的糖尿病肾病患者中,碳酸氢钠对肾脏纤维化和损伤标志物的影响尚不清楚。
设计、地点、参与者和测量方法:我们在美国进行了一项随机、双盲、安慰剂对照的研究,共纳入 74 名患有 1 型或 2 型糖尿病、肾小球滤过率(eGFR)为 15-89ml/min/1.73m、尿白蛋白与肌酐比值(UACR)≥30mg/g 和血清总 CO 为 22-28meq/L 的退伍军人。参与者每天接受口服碳酸氢钠(0.5meq/kg 瘦体重;=35)或安慰剂(=39)治疗 6 个月。主要结局是从基线到第 3 个月和第 6 个月时尿 TGF-1/肌酐的变化。次要结局包括从基线到第 3 个月和第 6 个月时尿肾损伤分子-1(KIM-1)/肌酐、纤连蛋白/肌酐、中性粒细胞明胶酶相关脂质运载蛋白(NGAL)/肌酐和 UACR 的变化。
关键的基线特征为年龄 72±8 岁,eGFR 为 51±18ml/min/1.73m,血清总 CO 为 24±2meq/L。碳酸氢钠治疗使平均总 CO 增加 1.2(95%置信区间[95%CI],0.3 至 2.1)meq/L,尿 pH 值增加 0.6(95%CI,0.5 至 0.8),尿铵排泄减少 5(95%CI,0 至 11)meq/d,尿可滴定酸排泄减少 11(95%CI,5 至 18)meq/d。碳酸氢钠治疗并未显著改变尿 TGF-1/肌酐(变化差异为 13%,95%CI,-10%至 40%;碳酸氢钠组内变化为 8%,95%CI,-10%至 28%;安慰剂组内变化为-4%,95%CI,-19%至 13%)。同样,尿 KIM-1/肌酐(变化差异为-10%,95%CI,-38%至 31%)、纤连蛋白/肌酐(8%,95%CI,-15%至 37%)、NGAL/肌酐(-33%,95%CI,-56%至 4%)或 UACR(1%,95%CI,-25%至 36%)也无明显变化。
在非酸中毒性糖尿病肾病患者中,碳酸氢钠治疗 6 个月并未显著降低尿 TGF-1、KIM-1、纤连蛋白、NGAL 或 UACR。