Liu Zhuo, Tang Shiying, Tian Xiaojun, Zhang Hongxian, Wang Guoliang, Zhang Shudong, Ma Lulin
Department of Urology, Peking University Third Hospital, 49 North Garden Rd., Haidian District, Beijing, People's Republic of China.
BMC Cancer. 2020 Jan 28;20(1):61. doi: 10.1186/s12885-020-6563-7.
To explore the influencing factors of perioperative renal function change and their relationship with prognosis on renal cell carcinoma (RCC) patients with tumor thrombus after nephrectomy and thrombectomy.
The clinical and pathological data of 135 patients with RCC and tumor thrombus, who underwent nephrectomy and thrombectomy at Peking University Third Hospital from May 2015 to July 2018, was retrospectively analyzed. Absolute change in estimated glomerular filtration rate (eGFR) (ACE) and percent change in eGFR (PCE) were calculated by preoperative and postoperative renal function. Linear regression analysis was used to explore the influencing factors of ACE and PCE, and logistic regression analysis was used to explore the influencing factors of worse postoperative renal function [eGFR≤60 mL/(min × 1.73 m^2)]. Cancer-specific survival (CSS) was estimated by Kaplan-Meier method and multivariate Cox regression, which were used to explore the effect of ACE and PCE on prognosis.
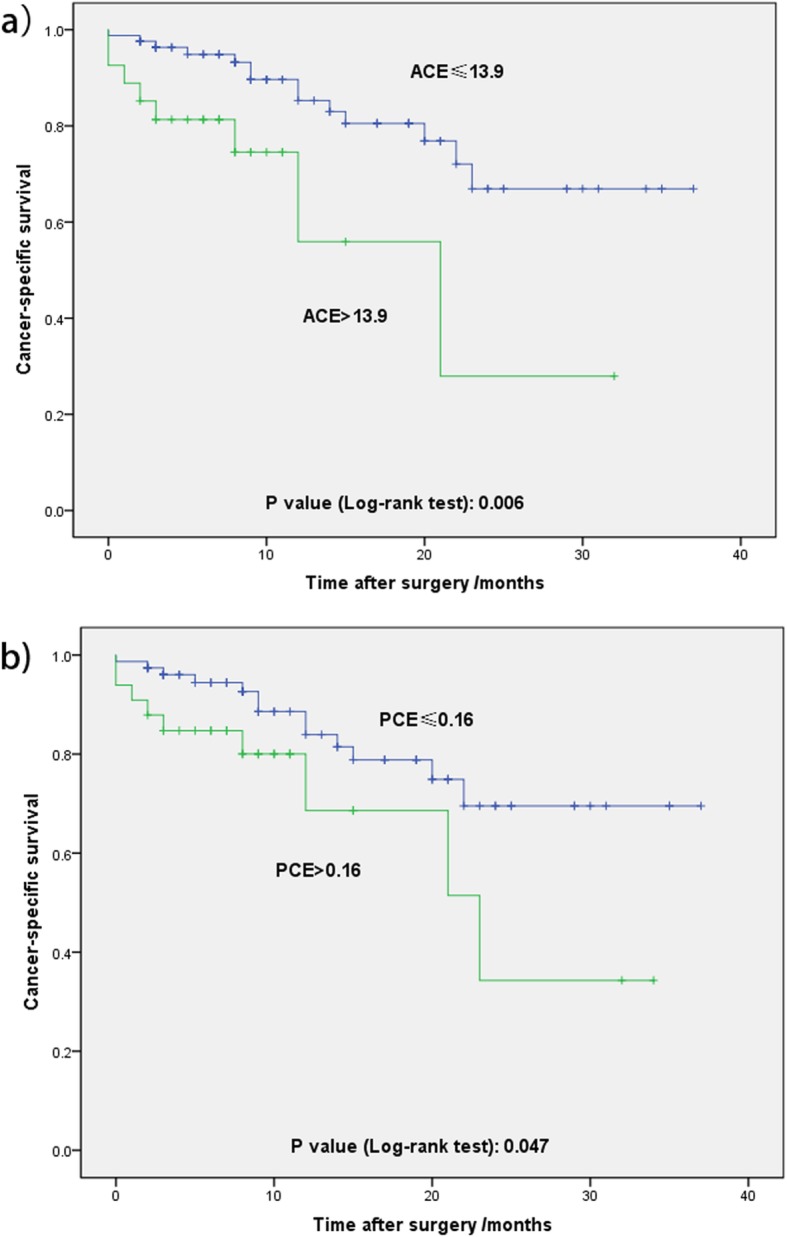
Of all the 135 patients, 101 patients (74.8%) were male and 34 patients (25.2%) were female. The mean preoperative eGFR was 73.9 ± 21.8 mL/(min × 1.73 m^2) and postoperative eGFR was 69.5 ± 25.2 mL/(min × 1.73 m^2). In multivariate linear regression analysis, preoperative eGFR (P < 0.001) and pathological type (P = 0.038) were significant predictive factors of ACE. In aspect of PCE, preoperative eGFR (P < 0.001) and pathological type (P = 0.002) were significant predictors. In multivariate logistic regression analysis, preoperative eGFR (P = 0.016) was the only risk factor of predicting worse postoperative renal function. During follow-up, 22 patients (16.3%) were dead due to RCC. According to ROC analysis, the cut off value of ACE and PCE was 13.9 and 0.16, respectively. ACE> 13.9 and PCE > 0.16 indicated worse CSS (P = 0.006 and P = 0.047, respectively). However, in multivariate Cox regression analysis of several related factors, perinephric tissues invasion (P = 0.001), sarcomatoid differentiation (P = 0.001) and ACE> 13.9 (P = 0.002) were significant prognostic factors for CSS. PCE > 0.16 seemed to be not (P = 0.055).
We explored several clinicopathological risk factors of predicting renal function change and their relationship with prognosis of RCC patients with tumor thrombus after nephrectomy and thrombectomy. The renal function change, which was associated with preoperative eGFR and pathological type, was prognostic risk factor for CSS and ACE> 13.9 indicated the worse prognosis.
探讨肾细胞癌(RCC)合并肿瘤血栓患者肾切除及血栓清除术后围手术期肾功能变化的影响因素及其与预后的关系。
回顾性分析2015年5月至2018年7月在北京大学第三医院接受肾切除及血栓清除术的135例RCC合并肿瘤血栓患者的临床和病理资料。根据术前和术后肾功能计算估计肾小球滤过率(eGFR)的绝对变化(ACE)和eGFR的百分比变化(PCE)。采用线性回归分析探讨ACE和PCE的影响因素,采用逻辑回归分析探讨术后肾功能恶化[eGFR≤60 mL/(min·1.73 m²)]的影响因素。采用Kaplan-Meier法和多因素Cox回归估计癌症特异性生存(CSS),并探讨ACE和PCE对预后的影响。
135例患者中,男性101例(74.8%),女性34例(25.2%)。术前eGFR平均为73.9±21.8 mL/(min·1.73 m²),术后eGFR为69.5±25.2 mL/(min·1.73 m²)。多因素线性回归分析显示,术前eGFR(P<0.001)和病理类型(P = 0.038)是ACE的显著预测因素。在PCE方面,术前eGFR(P<0.001)和病理类型(P = 0.002)是显著预测因素。多因素逻辑回归分析显示,术前eGFR(P = 0.016)是预测术后肾功能恶化的唯一危险因素。随访期间,22例(16.3%)患者死于RCC。根据ROC分析,ACE和PCE的截断值分别为13.9和0.16。ACE>13.9和PCE>0.16提示CSS较差(分别为P = 0.006和P = 0.047)。然而,在对多个相关因素的多因素Cox回归分析中,肾周组织侵犯(P = 0.001)、肉瘤样分化(P = 0.001)和ACE>13.9(P = 0.002)是CSS的显著预后因素。PCE>0.16似乎不是(P = 0.055)。
我们探讨了肾切除及血栓清除术后RCC合并肿瘤血栓患者预测肾功能变化的几个临床病理危险因素及其与预后的关系。与术前eGFR和病理类型相关的肾功能变化是CSS的预后危险因素,ACE>13.9提示预后较差。