Ruth M Rothstein CORE Center, Chicago, IL, United States of America.
Midway Research Center, Fort Pierce, FL, United States of America.
PLoS One. 2020 Jan 29;15(1):e0224875. doi: 10.1371/journal.pone.0224875. eCollection 2020.
Guidelines advocate the treatment of HCV in all HIV/HCV co-infected individuals. The aim of this randomized, open-label study (ClinicalTrials.gov identifier: NCT02707601; https://clinicaltrials.gov/ct2/show/NCT02707601) was to evaluate the safety/efficacy of ledipasvir/sofosbuvir (LDV/SOF) co-administered with elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (E/C/F/TAF) or rilpivirine/F/TAF (R/F/TAF) in HIV-1/HCV co-infected participants.
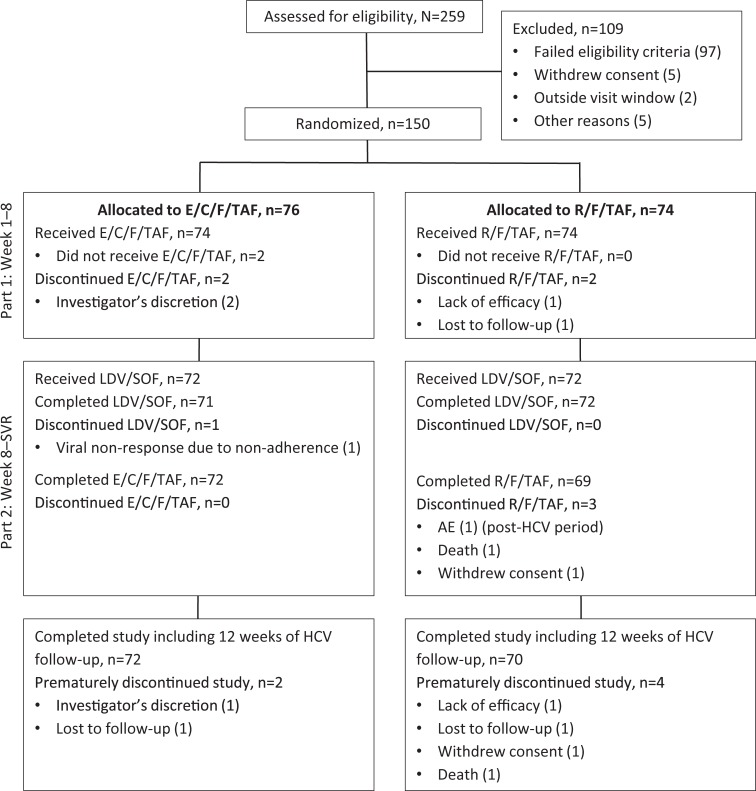
Participants with HIV-1 RNA <50 copies/mL and chronic HCV-genotype (GT) 1 (HCV treatment-naïve ± compensated cirrhosis or HCV treatment-experienced non-cirrhotic) were randomized 1:1 to switch to E/C/F/TAF or R/F/TAF. If HIV suppression was maintained at Week 8, participants received 12 weeks of LDV/SOF. The primary endpoint was sustained HCV virologic response 12 weeks after LDV/SOF completion (SVR12).
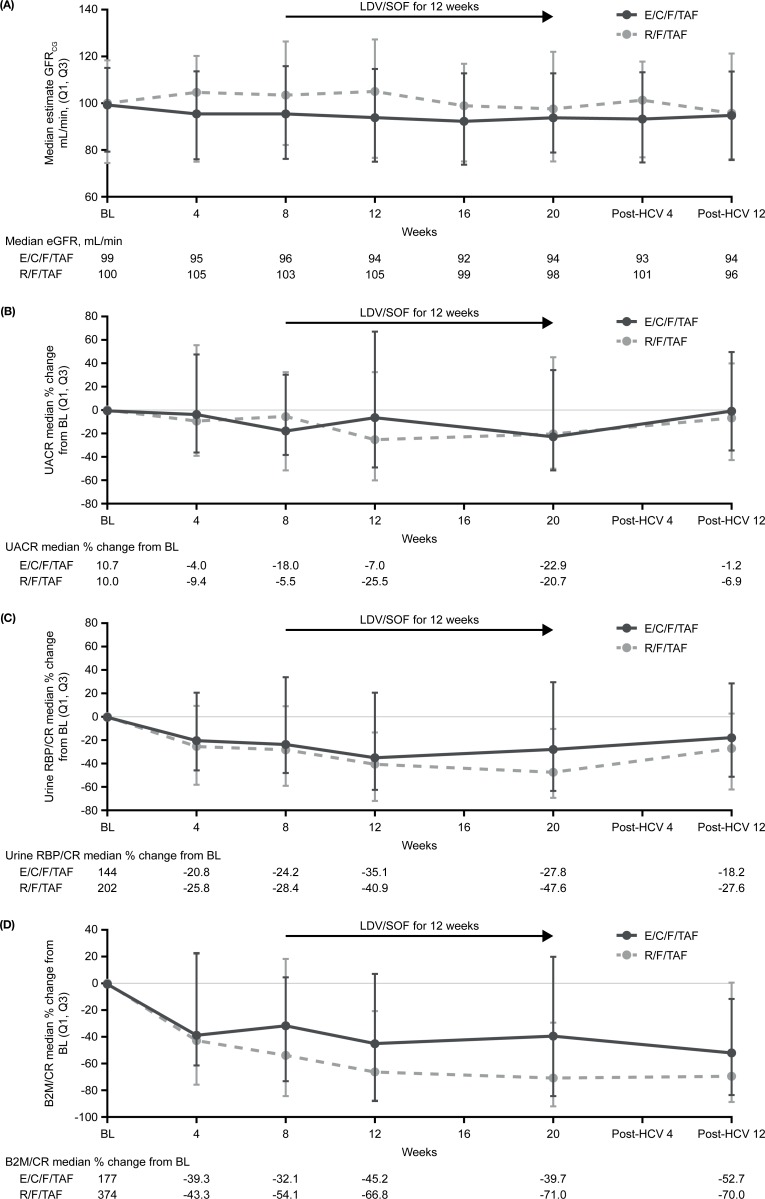
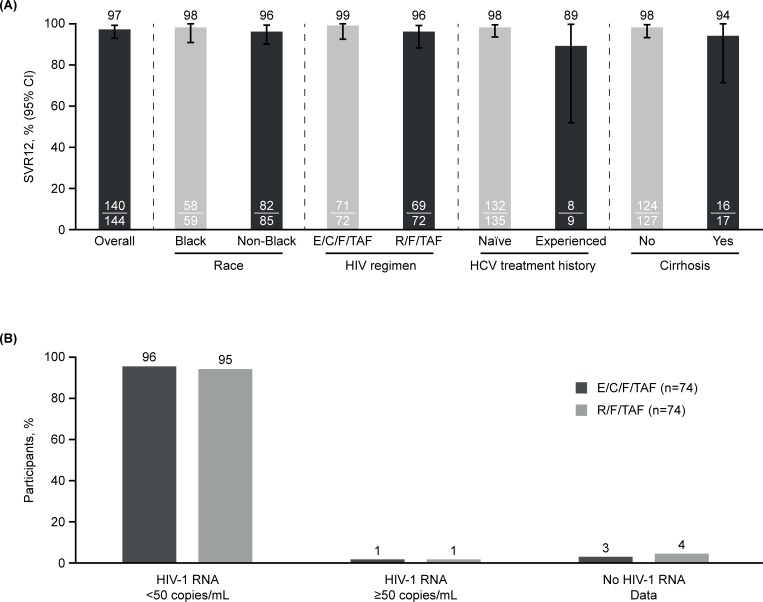
Of 150 participants, 148 received ≥1 dose of HIV study drug and 144 received LDV/SOF (72 in each F/TAF group; 83% GT1a, 94% HCV treatment-naïve, 12% cirrhotic). Overall, SVR12 was 97% (95% confidence interval: 93-99%). Black race did not affect SVR12. Of four participants not achieving SVR12, one had HCV relapse, one had HCV virologic non-response due to non-adherence, and two missed the post-HCV Week 12 visit. Of 148 participants, 96% receiving E/C/F/TAF and 95% receiving R/F/TAF maintained HIV suppression at Week 24; no HIV resistance was detected. No participant discontinued LDV/SOF or E/C/F/TAF due to adverse events; one participant discontinued R/F/TAF due to worsening of pre-existing hypercholesterolemia. Renal toxicity was not observed in either F/TAF regimen during LDV/SOF co-administration. In conclusion, high rates of HCV SVR12 and maintenance of HIV suppression were achieved with LDV/SOF and F/TAF-based regimens.
This study supports LDV/SOF co-administered with an F/TAF-based regimen in HIV-1/HCV-GT1 co-infected patients.
指南主张对所有 HIV/HCV 合并感染的个体进行 HCV 治疗。本随机、开放标签研究(ClinicalTrials.gov 标识符:NCT02707601;https://clinicaltrials.gov/ct2/show/NCT02707601)旨在评估 ledipasvir/sofosbuvir(LDV/SOF)与elvitegravir/cobicistat/恩曲他滨/替诺福韦艾拉酚胺(E/C/F/TAF)或 rilpivirine/F/TAF(R/F/TAF)联合用于 HIV-1/HCV 合并感染参与者的安全性/疗效。
HIV-1 RNA<50 拷贝/mL 且慢性 HCV 基因型(GT)1(HCV 初治±代偿性肝硬化或 HCV 经治非肝硬化)的参与者以 1:1 的比例随机分配至转换为 E/C/F/TAF 或 R/F/TAF。如果在第 8 周维持 HIV 抑制,参与者接受 12 周的 LDV/SOF。主要终点是 LDV/SOF 完成后 12 周的持续 HCV 病毒学应答(SVR12)。
在 150 名参与者中,148 名接受了至少 1 剂 HIV 研究药物,144 名接受了 LDV/SOF(每组 F/TAF 组 72 名;83% GT1a,94% HCV 初治,12%肝硬化)。总体而言,SVR12 为 97%(95%置信区间:93-99%)。黑人种族并不影响 SVR12。4 名未达到 SVR12 的参与者中,1 名发生 HCV 复发,1 名因不依从而发生 HCV 病毒学无应答,2 名错过 HCV 治疗后第 12 周的访视。在 148 名参与者中,96%接受 E/C/F/TAF 和 95%接受 R/F/TAF 的患者在第 24 周维持 HIV 抑制;未检测到 HIV 耐药性。没有参与者因不良反应而停止 LDV/SOF 或 E/C/F/TAF;1 名参与者因先前存在的高胆固醇血症恶化而停止 R/F/TAF。在 LDV/SOF 联合治疗期间,两种 F/TAF 方案均未观察到肾毒性。总之,在 HIV-1/HCV-GT1 合并感染患者中,LDV/SOF 联合 F/TAF 方案可实现高 HCV SVR12 和 HIV 抑制的维持。
本研究支持在 HIV-1/HCV-GT1 合并感染患者中使用 LDV/SOF 联合 F/TAF 方案。