Division of Global Women's Health, Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, United States of America.
Department of Obstetrics and Gynaecology, University of Zambia School of Medicine, Lusaka, Zambia.
PLoS One. 2020 Jan 29;15(1):e0224874. doi: 10.1371/journal.pone.0224874. eCollection 2020.
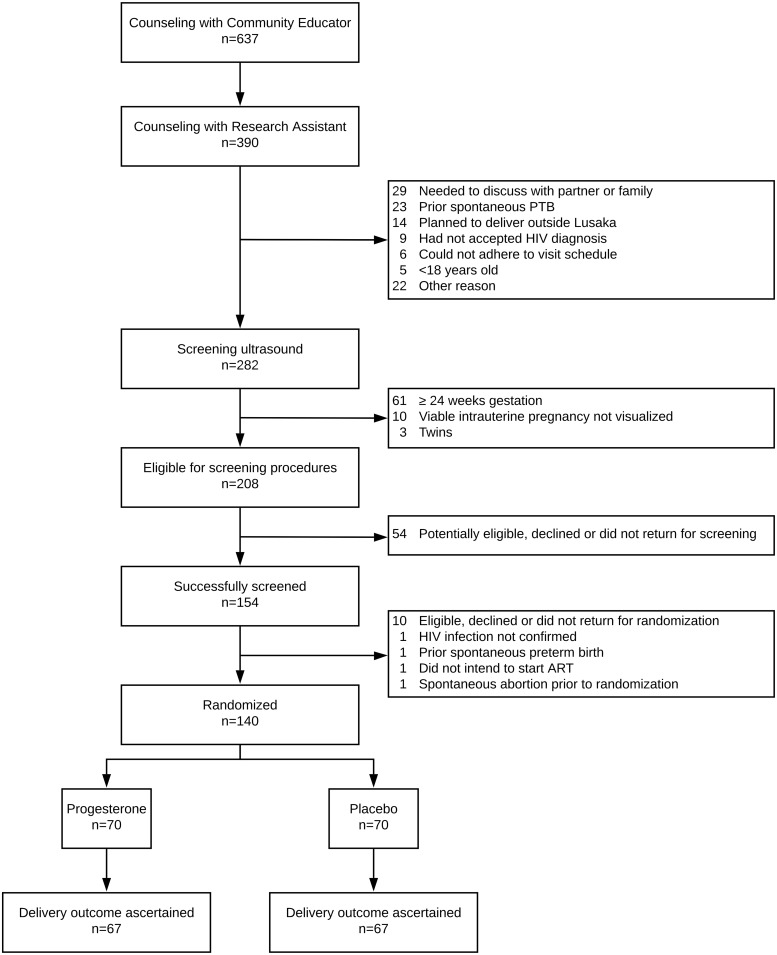
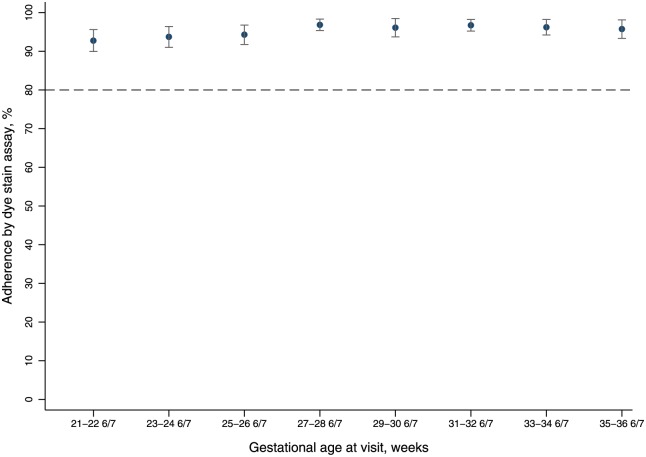
Antenatal vaginal progesterone (VP) reduces the risk of preterm birth (PTB) in women with shortened cervical length, and we hypothesize that it may also prevent PTB in women with HIV as their primary risk factor. We conducted a pilot feasibility study in Lusaka, Zambia to investigate uptake, adherence, and retention in preparation for a future efficacy trial. This was a double-masked, placebo-controlled, randomized trial of 200mg daily self-administered VP suppository or placebo. Pregnant women with HIV who were initiating or continuing antiretroviral therapy were eligible for participation. Potential participants underwent ultrasound to assess eligibility; we excluded those ≥24 gestational weeks, with non-viable, multiple gestation, or extrauterine pregnancies, with short cervix (<2.0cm), or with prior spontaneous PTB. Participants initiated study product between 20-24 weeks of gestation and continued to 37 weeks (or delivery, if sooner). The primary outcome was adherence (proportion achieving ≥80% study product use), assessed by dye stain assay of returned single-use vaginal applicators. Secondary outcomes with pre-defined feasibility targets were: uptake (≥50% eligible participants enrolled) and retention (≥90% ascertainment of delivery outcomes). We also evaluated preliminary efficacy by comparing the risk of spontaneous PTB <37 weeks between groups. From July 2017 to June 2018, 208 HIV-infected pregnant women were eligible for screening and 140 (uptake = 67%) were randomly allocated to VP (n = 70) or placebo (n = 70). Mean adherence was 94% (SD±9.4); 91% (n = 125/137) achieved overall adherence ≥80%. Delivery outcomes were ascertained from 134 (96%) participants. Spontaneous PTB occurred in 10 participants (15%) receiving placebo and 8 (12%) receiving progesterone (RR 0.82; 95%CI:0.34-1.97). Spontaneous PTB < 34 weeks occurred in 6 (9%) receiving placebo and 4 (6%) receiving progesterone (RR 0.67; 95%CI:0.20-2.67). In contrast to findings from vaginal microbicide studies in HIV-uninfected, non-pregnant women, our trial participants were highly adherent to daily self-administered vaginal progesterone. The study's a priori criteria for uptake, adherence, and retention were met, indicating that a phase III efficacy trial would be feasible.
产前阴道用黄体酮(VP)可降低宫颈长度缩短的孕妇早产(PTB)的风险,我们假设它也可以预防 HIV 作为主要风险因素的孕妇早产。我们在赞比亚卢萨卡进行了一项试点可行性研究,为未来的疗效试验做准备,以调查接受度、依从性和保留率。这是一项 200mg 每日自行阴道给药 VP 栓剂或安慰剂的双盲、安慰剂对照、随机试验。正在开始或继续抗逆转录病毒治疗的 HIV 孕妇有资格参加。潜在的参与者接受了超声检查以评估合格性;我们排除了那些≥24 孕周、无活力、多胎或子宫外妊娠、宫颈短(<2.0cm)或既往自发性早产的孕妇。参与者在 20-24 孕周开始研究产品,并持续到 37 孕周(或分娩,如果更早)。主要结局是通过返回的单次使用阴道给药器的染料染色测定来评估的依从性(达到≥80%研究产品使用的比例)。具有预定义可行性目标的次要结局是:接受度(≥50%合格参与者入组)和保留率(≥90%确定分娩结局)。我们还通过比较两组自发性 PTB<37 周的风险来评估初步疗效。2017 年 7 月至 2018 年 6 月,有 208 名 HIV 感染孕妇符合筛查条件,其中 140 名(接受度=67%)被随机分配至 VP(n=70)或安慰剂(n=70)。平均依从率为 94%(SD±9.4);91%(n=125/137)达到了总体依从性≥80%。从 134 名(96%)参与者中确定了分娩结局。接受安慰剂的 10 名参与者(15%)和接受孕激素的 8 名参与者(12%)发生自发性早产(RR 0.82;95%CI:0.34-1.97)。接受安慰剂的 6 名参与者(9%)和接受孕激素的 4 名参与者(6%)发生自发性 PTB<34 周(RR 0.67;95%CI:0.20-2.67)。与 HIV 未感染、非孕妇阴道杀微生物剂研究的发现相反,我们的试验参与者对每日自行阴道给予孕激素的依从性很高。研究的接受度、依从性和保留率符合事先设定的标准,表明 III 期疗效试验是可行的。