School of Health and Related Research (ScHARR) University of Sheffield, Regent Court, 30 Regent Street, Sheffield, S1 4DA, UK.
Nottingham Clinical Trials Unit (NCTU), University of Nottingham, Nottingham, UK.
Trials. 2020 Jan 29;21(1):116. doi: 10.1186/s13063-019-3807-4.
Group interventions are interventions delivered to groups of people rather than to individuals and are used in healthcare for mental health recovery, behaviour change, peer support, self-management and/or health education. Evaluating group interventions in randomised controlled trials (RCTs) presents trialists with a set of practical problems, which are not present in RCTs of one-to-one interventions and which may not be immediately obvious.
Case-based approach summarising Sheffield trials unit's experience in the design and implementation of five group interventions. We reviewed participant recruitment and attrition, facilitator training and attrition, attendance at the group sessions, group size and fidelity aspects across five RCTs.
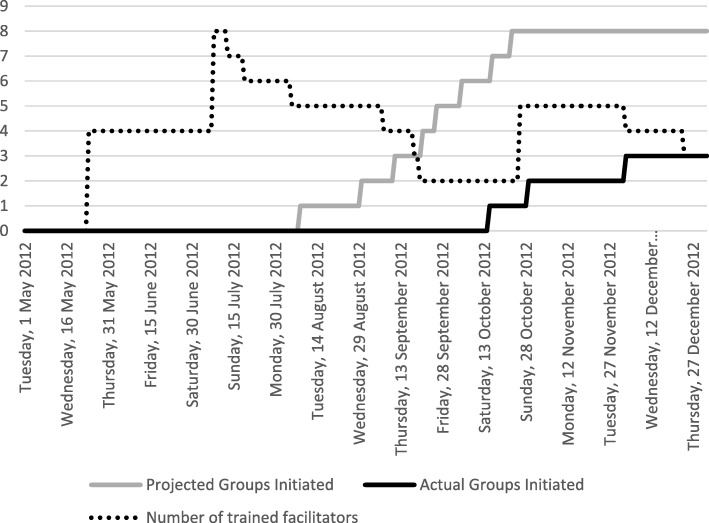
Median recruitment across the five trials was 3.2 (range 1.7-21.0) participants per site per month. Group intervention trials involve a delay in starting the intervention for some participants, until sufficient numbers are available to start a group. There was no evidence that the timing of consent, relative to randomisation, affected post-randomisation attrition which was a matter of concern for all trial teams. Group facilitator attrition was common in studies where facilitators were employed by the health system rather than the by the grant holder and led to the early closure of one trial; research sites responded by training 'back-up' and new facilitators. Trials specified that participants had to attend a median of 62.5% (range 16.7%-80%) of sessions, in order to receive a 'therapeutic dose'; a median of 76.7% (range 42.9%-97.8%) received a therapeutic dose. Across the five trials, 75.3% of all sessions went ahead without the pre-specified ideal group size. A variety of methods were used to assess the fidelity of group interventions at a group and individual level across the five trials.
This is the first paper to provide an empirical basis for planning group intervention trials. Investigators should expect delays/difficulties in recruiting groups of the optimal size, plan for both facilitator and participant attrition, and consider how group attendance and group size affects treatment fidelity.
ISRCTN17993825 registered on 11/10/2016, ISRCTN28645428 registered on 11/04/2012, ISRCTN61215213 registered on 11/05/2011, ISRCTN67209155 registered on 22/03/2012, ISRCTN19447796 registered on 20/03/2014.
团体干预是指针对人群而非个体提供的干预措施,在心理健康恢复、行为改变、同伴支持、自我管理和/或健康教育等领域用于医疗保健。在随机对照试验 (RCT) 中评估团体干预存在一系列实际问题,这些问题在一对一干预的 RCT 中不存在,也可能不那么明显。
基于案例的方法总结了谢菲尔德试验单位在设计和实施五组干预措施方面的经验。我们回顾了五个 RCT 中的参与者招募和脱落、培训师培训和脱落、小组会议出席情况、小组规模和保真度方面的情况。
五个试验的中位数招募率为每个站点每月 3.2 名(范围 1.7-21.0)参与者。团体干预试验涉及到一些参与者开始干预的延迟,直到有足够的人数可以开始一个小组。没有证据表明同意的时间相对于随机分组会影响随机分组后的脱落,这是所有试验团队都关心的问题。在研究中,培训师是由卫生系统而不是赠款持有者雇用的情况下,培训师的脱落很常见,这导致了一项试验的提前关闭;研究地点通过培训“后备”和新的培训师做出了回应。试验规定,参与者必须参加中位数为 62.5%(范围 16.7%-80%)的课程,以获得“治疗剂量”;中位数为 76.7%(范围 42.9%-97.8%)接受了治疗剂量。在五个试验中,75.3%的所有课程都在没有预定理想小组规模的情况下进行。在五个试验中,使用了各种方法来评估小组干预的小组和个人层面的保真度。
这是第一份为规划团体干预试验提供实证依据的论文。研究人员应预计会遇到招募最佳规模小组的延迟/困难,计划培训师和参与者的脱落,并考虑小组出勤率和小组规模如何影响治疗的保真度。
ISRCTN17993825 于 2016 年 10 月 11 日注册,ISRCTN28645428 于 2012 年 11 月 4 日注册,ISRCTN61215213 于 2011 年 11 月 5 日注册,ISRCTN67209155 于 2012 年 11 月 22 日注册,ISRCTN19447796 于 2014 年 3 月 20 日注册。