Department of Stereotactic and Functional Neurosurgery, Freiburg University Medical Center, Freiburg (i.Br.), Germany.
Faculty of Medicine, Freiburg University, Freiburg (i.Br.), Germany.
Acta Neurochir (Wien). 2020 May;162(5):1053-1066. doi: 10.1007/s00701-020-04248-2. Epub 2020 Jan 29.
Deep brain stimulation alleviates tremor of various origins. The dentato-rubro-thalamic tract (DRT) has been suspected as a common tremor-reducing structure. Statistical evidence has not been obtained. We here report the results of an uncontrolled case series of patients with refractory tremor who underwent deep brain stimulation under tractographic assistance.
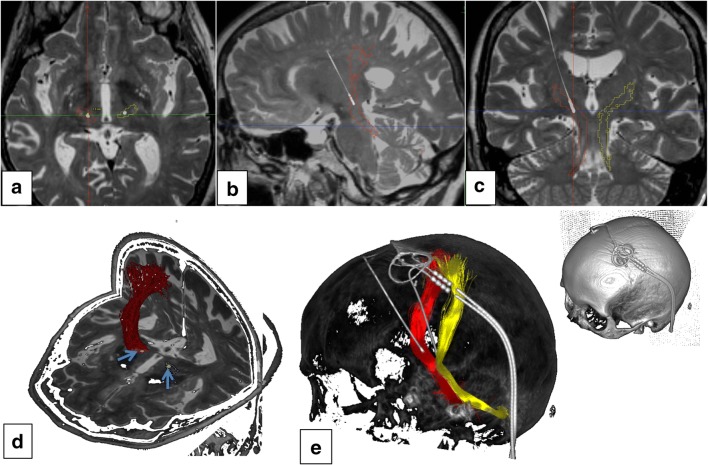
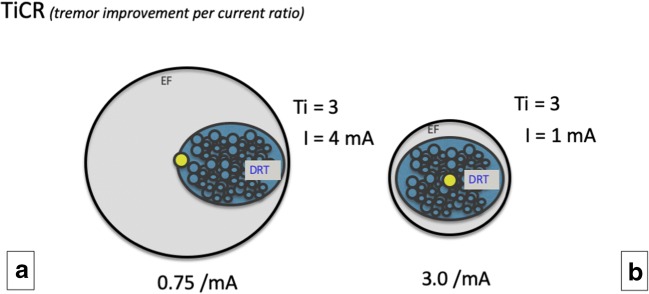
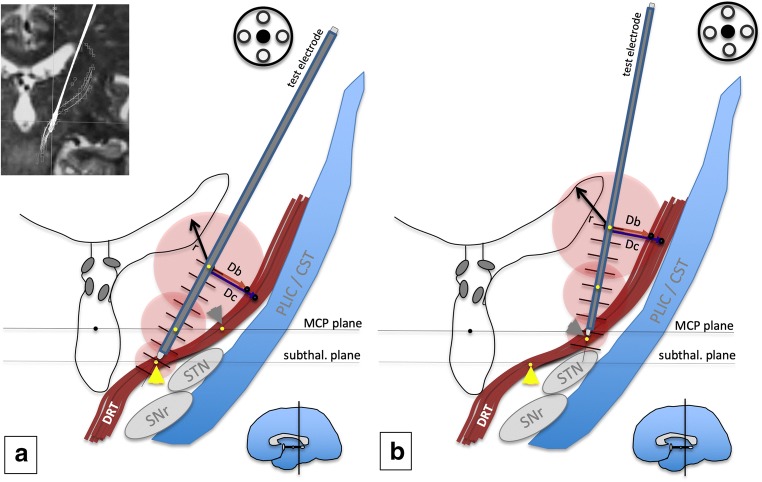
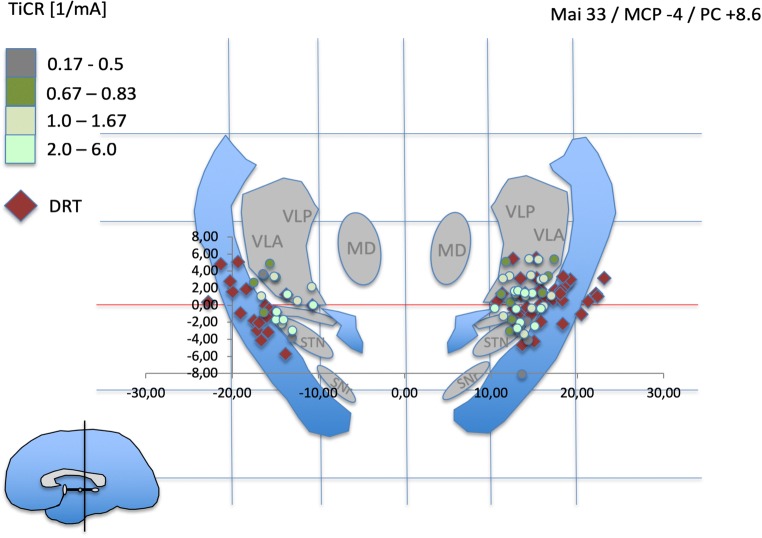
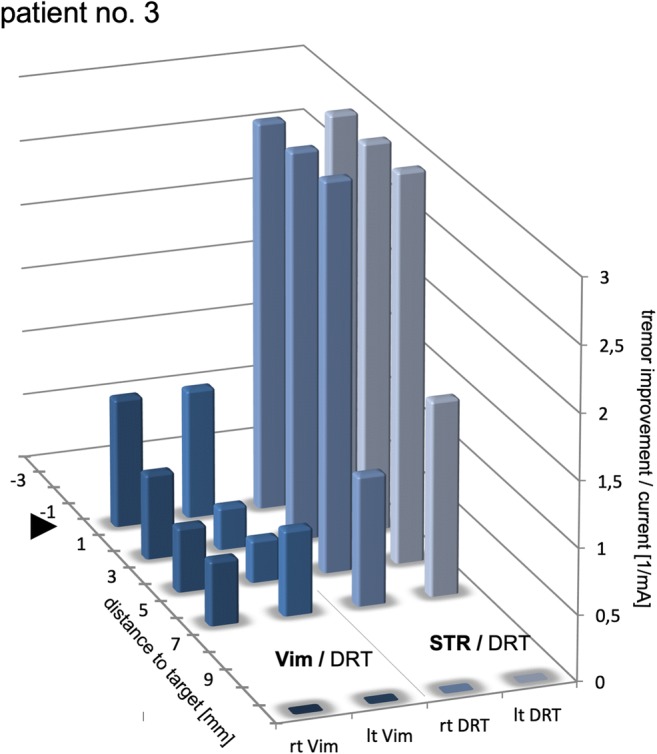
A total of 36 patients were enrolled (essential tremor (17), Parkinson's tremor (8), multiple sclerosis (7), dystonic head tremor (3), tardive dystonia (1)) and received 62 DBS electrodes (26 bilateral; 10 unilateral). Preoperatively, diffusion tensor magnetic resonance imaging sequences were acquired together with high-resolution anatomical T1W and T2W sequences. The DRT was individually tracked and used as a direct thalamic or subthalamic target. Intraoperative tremor reduction was graded on a 4-point scale (0 = no tremor reduction to 3 = full tremor control) and recorded together with the current amplitude, respectively. Stimulation point coordinates were recorded and compared to DRT. The relation of the current amplitude needed to reduce tremor was expressed as TiCR (tremor improvement per current ratio).
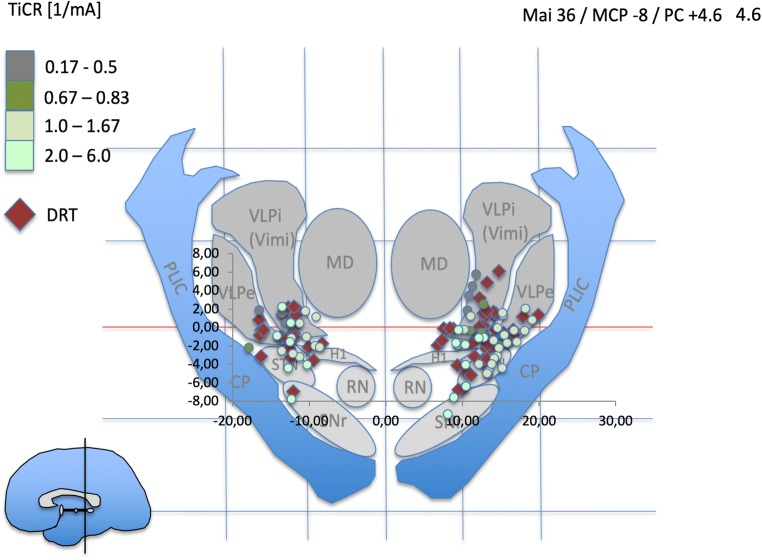
Stimulation points of 241 were available for analysis. A total of 68 trajectories were tested (62 dB leads, 1.1 trajectories tested per implanted lead). Tremor improvement was significantly decreasing (p < 0.01) if the distance to both the border and the center of the DRT was increasing. On the initial trajectory, 56 leads (90.3%) were finally placed. Long-term outcomes were not part of this analysis.
Tremor of various origins was acutely alleviated at different points along the DRT fiber tract (above and below the MCP plane) despite different tremor diseases. DRT is potentially a common tremor-reducing structure. Individual targeting helps to reduce brain penetrating tracts. TiCR characterizes stimulation efficacy and might help to identify an optimal stimulation point.
深部脑刺激可缓解各种来源的震颤。齿状核红核丘脑束(DRT)被怀疑是一种常见的震颤减轻结构。但是尚未获得统计学证据。我们在此报告了在轨迹引导下接受深部脑刺激的难治性震颤患者的无对照病例系列结果。
共纳入 36 例患者(特发性震颤(17),帕金森震颤(8),多发性硬化症(7),肌张力障碍性头部震颤(3),迟发性运动障碍(1)),并接受了 62 个 DBS 电极(26 个双侧;10 个单侧)。术前采集弥散张量磁共振成像序列以及高分辨率解剖 T1W 和 T2W 序列。单独跟踪 DRT 并将其用作直接丘脑或丘脑下靶点。术中震颤减少程度按 4 分制(0=无震颤减少,3=完全震颤控制)分级,并分别记录电流幅度。记录刺激点坐标并与 DRT 进行比较。表示震颤改善与电流比的 TiCR(每电流震颤改善比)来表示减少震颤所需的电流幅度的关系。
可用于分析的刺激点有 241 个。共测试了 68 条轨迹(62 个 dB 导联,每个植入导联测试 1.1 条轨迹)。如果距离 DRT 的边界和中心都增加,则震颤改善明显减少(p <0.01)。在初始轨迹上,最终放置了 56 个导联(90.3%)。长期结果不是本分析的一部分。
尽管震颤疾病不同,但沿 DRT 纤维束(MCP 平面上方和下方)的不同点可急性缓解各种来源的震颤。DRT 可能是一种常见的震颤减轻结构。个体化靶向有助于减少脑穿透轨迹。TiCR 可表征刺激效果,并有助于确定最佳刺激点。