1st Department of Internal Medicine, University Medical Hospital Hamburg-Eppendorf, Martinistr 52, 20246, Hamburg, Germany.
German Center for Infection Research (DZIF), Hamburg-Lübeck-Borstel site, Hamburg, Germany.
BMC Gastroenterol. 2020 Jan 30;20(1):24. doi: 10.1186/s12876-020-1168-9.
Chronic hepatitis delta virus (HDV) infection causes severe liver disease which often leads to cirrhosis and hepatocellular carcinoma (HCC). Aim of this study was to establish the disease severity and prognostic factors for disease outcome by analysing frequencies of clinical events and their correlation with baseline virological and biochemical parameters as well as interferon and nucleos(t)ide analogue treatment choice.
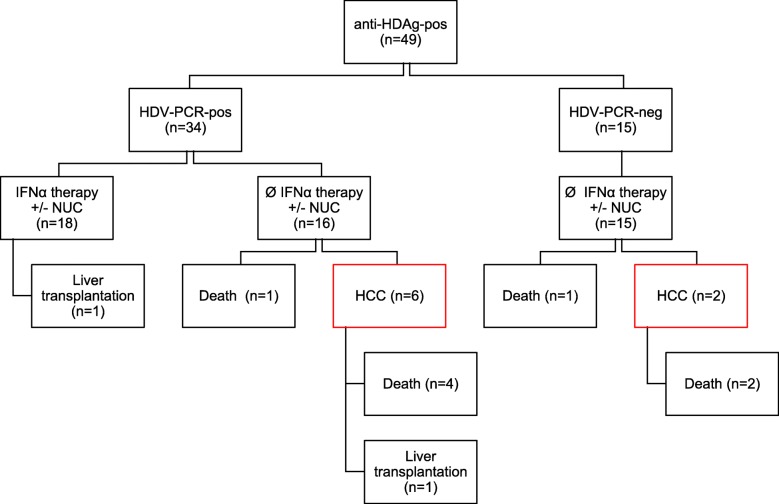
We studied a single-centre cohort of 49 anti-HDAg-positive patients with HBsAg persistence for at least 6 months. Virological and biochemical parameters, interferon and nucleos(t)ide analogue treatment choice as well as clinical events during follow-up were analysed by retrospective chart review (mean follow-up time 3 years, range 0.25-7.67 years).
Severe clinical events occurred in 11/49 hepatitis D patients, including HCC (8/49), death (8/49) or liver transplantation (2/49). HCCs only occurred secondary to liver cirrhosis and their event rates in this cohort of hepatitis D patients did not differ from a matched HBV mono-infected cohort with comparable frequency of liver cirrhosis. A stepwise multivariate logistic regression revealed low platelet count (p = 0. 0290) and older age (p = 0.0337) correlating most strongly with overall clinical events, while serum HDV RNA positivity at baseline did not correlate with any clinical outcome. Interferon-free but not nucleos(t)ide analogue-free patient care correlated with the occurrence of HCC at logistic regression, although only 3/18 interferon-treated patients demonstrated repeatedly negative HDV PCR results post therapy.
Our data indicate that progressive liver disease at baseline plays a major role as predictive factor for overall clinical outcome of hepatitis D patients. In particular, HCC risk may not be underestimated in hepatitis D virus RNA negative hepatitis D patients with advanced liver fibrosis.
慢性丁型肝炎病毒(HDV)感染可导致严重的肝脏疾病,通常导致肝硬化和肝细胞癌(HCC)。本研究的目的是通过分析临床事件的频率及其与基线病毒学和生化参数以及干扰素和核苷(酸)类似物治疗选择的相关性,来确定疾病严重程度和疾病结局的预测因素。
我们研究了一个由 49 名抗-HDAg 阳性、HBsAg 持续至少 6 个月的患者组成的单中心队列。通过回顾性病历分析(平均随访时间为 3 年,范围为 0.25-7.67 年),分析病毒学和生化参数、干扰素和核苷(酸)类似物治疗选择以及随访期间的临床事件。
49 例丁型肝炎患者中有 11 例发生严重临床事件,包括 HCC(8/49)、死亡(8/49)或肝移植(2/49)。HCC 仅继发于肝硬化,并且在该丁型肝炎患者队列中,其发生率与具有相似肝硬化频率的乙型肝炎病毒单感染队列无差异。逐步多变量逻辑回归显示,血小板计数低(p=0.0290)和年龄较大(p=0.0337)与总体临床事件相关性最强,而基线时血清 HDV RNA 阳性与任何临床结局均无相关性。无干扰素和无核苷(酸)类似物治疗的患者护理与 HCC 的发生相关,但仅 3/18 例接受干扰素治疗的患者在治疗后反复出现 HDV PCR 结果阴性。
我们的数据表明,基线时进行性肝脏疾病是预测丁型肝炎患者总体临床结局的主要因素。特别是,在 RNA 阴性的丁型肝炎病毒感染且有晚期纤维化的患者中,HCC 风险可能不会被低估。