Altreuther Martin, Mattsson Erney
Department of Vascular Surgery, St. Olav's Hospital, Trondheim University Hospital, Trondheim, Norway.
Department of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway.
SAGE Open Med. 2020 Jan 15;8:2050312119900860. doi: 10.1177/2050312119900860. eCollection 2020.
This population-based retrospective cohort study investigates long-term results of femoral thrombendarterectomy combined with simultaneous endovascular intervention of the iliac or femoropopliteal vessels, or both, with focus on freedom from recurrent intervention, limb salvage and survival.
All patients undergoing femoral thrombendarterectomy and simultaneous endovascular intervention between 1999 and 2013 were included. Stratification was according to clinical symptoms, intermittent claudication or critical ischemia, with subgroups for rest pain and ulcer/gangrene, and for type of endovascular intervention, iliac, femoropopliteal or both. We assessed technical success, 30-day complications, freedom from recurrent intervention, survival and amputation free survival in all patients. Limb salvage was assessed in patients with critical ischemia.
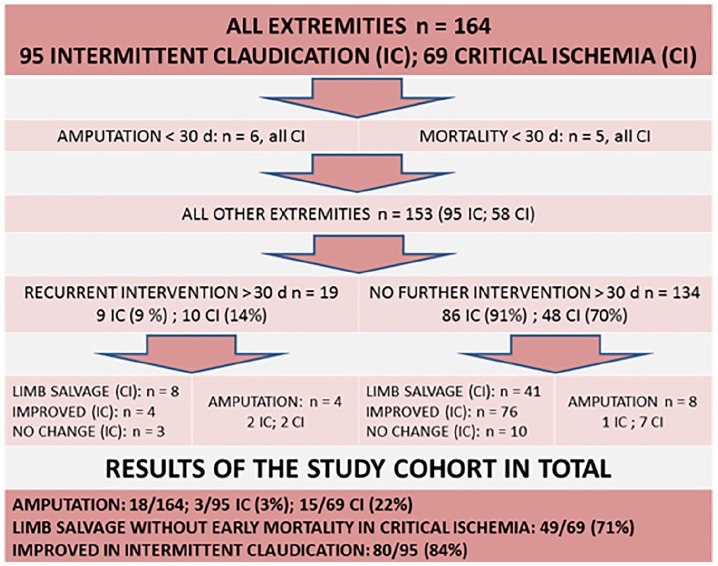
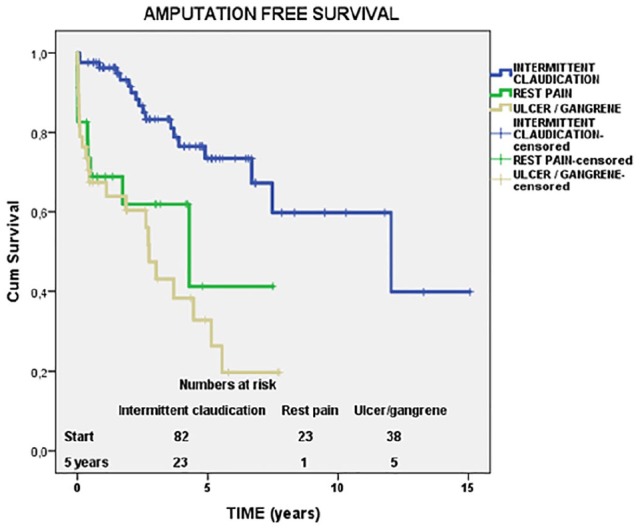
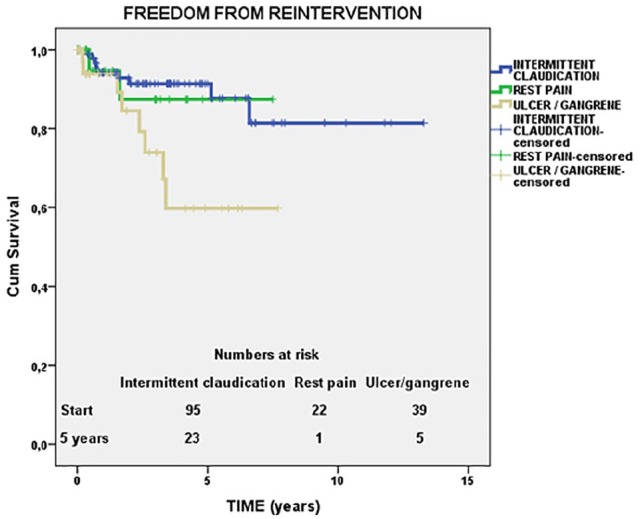
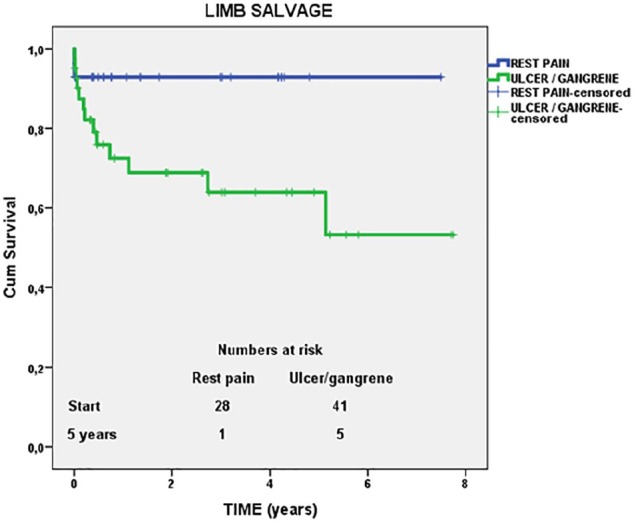
We identified 151 operations in 143 patients with a total of 164 limbs treated. A total of 13 patients had bilateral and 8 patients had subsequent contralateral operations. Indication was intermittent claudication in 87 (57.6%) and critical ischemia in 64 (42.4%) operations. Thirty-day mortality, only observed in critical ischemia, was 5/64 (7.8%). Freedom from recurrent intervention after 5 years was 91% in intermittent claudication and 70% in critical ischemia. In total, 84% of the patients with claudication were improved at the end of the study. Limb salvage at 5 years was 75% in critical ischemia, 93% in rest pain and 64% in patients with ulcer or gangrene.
Femoral thrombendarterectomy combined with endovascular iliac or femoropopliteal intervention has good and durable results in intermittent claudication and critical ischemia, especially in patients with rest pain. In most cases, a single operation is sufficient.
这项基于人群的回顾性队列研究调查了股动脉血栓内膜切除术联合髂血管或股腘血管(或两者)同期血管内介入治疗的长期结果,重点关注免于再次干预、肢体挽救和生存情况。
纳入1999年至2013年间接受股动脉血栓内膜切除术及同期血管内介入治疗的所有患者。根据临床症状分层,分为间歇性跛行或严重缺血,并进一步细分休息时疼痛和溃疡/坏疽亚组,同时根据血管内介入治疗类型分层,分为髂血管、股腘血管或两者。我们评估了所有患者的技术成功率、30天并发症、免于再次干预情况、生存率和无截肢生存率。对严重缺血患者评估肢体挽救情况。
我们确定了143例患者的151次手术,共治疗164条肢体。共有13例患者接受了双侧手术,8例患者随后接受了对侧手术。手术指征为间歇性跛行87例(57.6%),严重缺血64例(42.4%)。仅在严重缺血患者中观察到30天死亡率为5/64(7.8%)。间歇性跛行患者5年后免于再次干预的比例为91%,严重缺血患者为70%。总体而言,84%的间歇性跛行患者在研究结束时症状改善。严重缺血患者5年时的肢体挽救率为75%,休息时疼痛患者为93%,溃疡或坏疽患者为64%。
股动脉血栓内膜切除术联合髂血管或股腘血管血管内介入治疗在间歇性跛行和严重缺血患者中,尤其是休息时疼痛患者中,具有良好且持久的效果。在大多数情况下,单次手术就足够了。