Division of Nuclear Medicine, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria.
Department of Nuclear Medicine, Molecular Imaging and Special Endocrinology, University Hospital St. Pölten-Karl Landsteiner University of Health Science, St. Pölten, Austria.
Wien Klin Wochenschr. 2021 Feb;133(3-4):107-117. doi: 10.1007/s00508-020-01610-3. Epub 2020 Feb 3.
Donor kidney function is considered a critical determinant of allograft survival after live donor (LD) kidney transplantation, but its independent impact on the evolution of graft function is less well defined. The objective of this study was to dissect the relative contribution of LD kidney function to baseline estimated glomerular filtration rate (eGFR) of recipients and its decline.
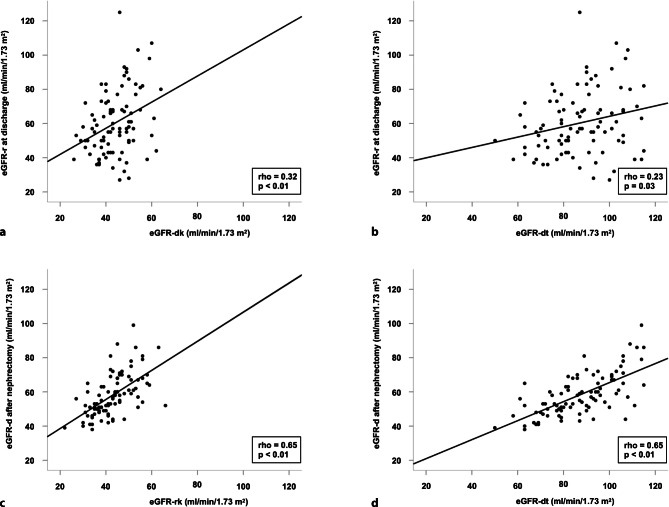
In this study 91 LD kidney transplantations performed between 2007 and 2015 were included. The eGFR of donated kidneys (eGFR-dk) was calculated from total LD eGFR (eGFR-dt) based on the results of isotope nephrography. Recipient eGFR (eGFR-r) determined 6‑monthly until 36 months posttransplantation served as dependent variable in mixed linear models estimating changes in baseline allograft function (intercept) and eGFR‑r slope. Models were adjusted either for eGFR-dk or eGFR-dt, in addition to other potential confounders.
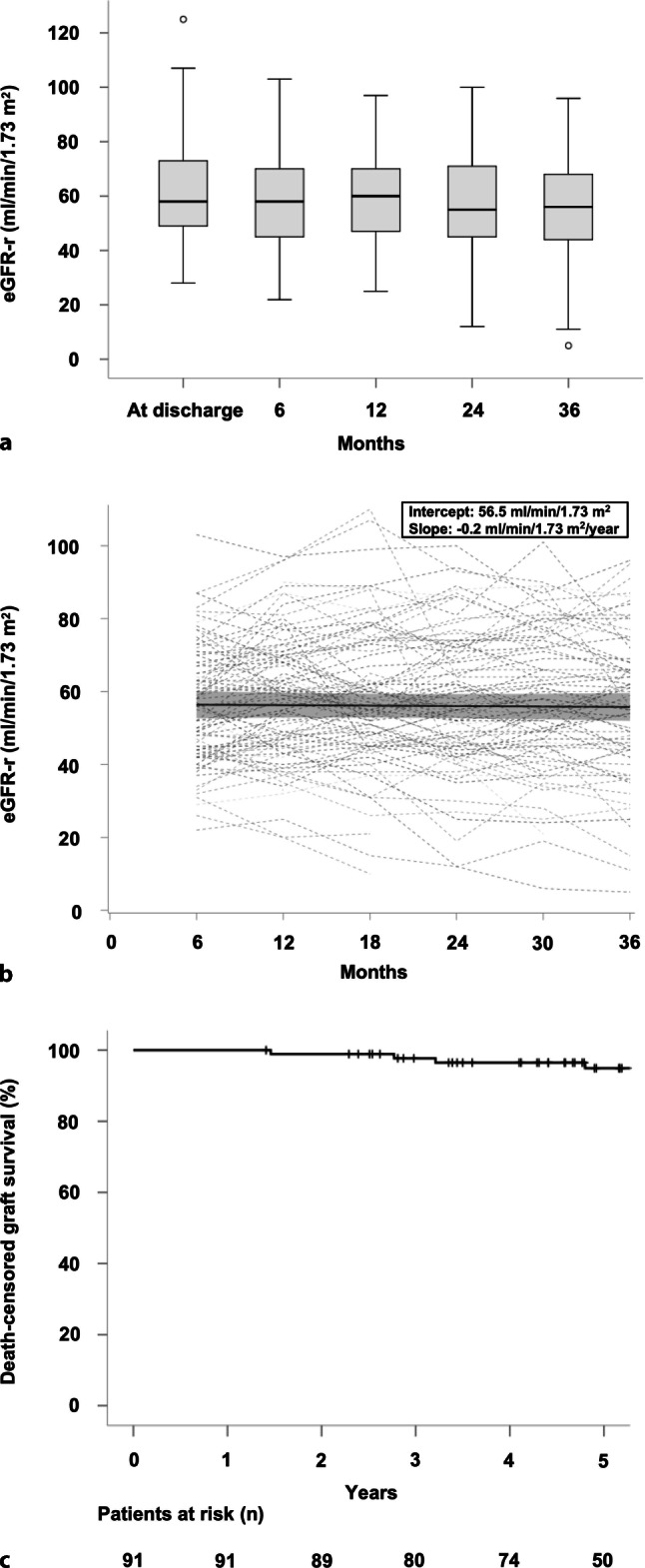
Overall, unadjusted mean eGFR‑r at baseline (6 months) and its annual decline in allograft function were 56.5 mL/min/1.73 m and -0.2 mL/min/1.73 m, respectively. In multivariate analysis, eGFR-dk impacted on baseline eGFR‑r (0.6 mL/min/1.73 m mean estimated increase per unit; P = 0.02) but not on its slope. In the eGFR-dt-adjusted model, a marginal effect was observed for LD age (P = 0.05). Both models identified antibody-mediated rejection (ABMR) as the strongest risk factor of accelerated loss of allograft function (eGFR‑r slope: approximately -6 mL/min/1.73 m per year; P ≤ 0.02).
Donor-related characteristics, most prominently the function of donated kidneys and LD age, were predictive of eGFR at baseline. The ABMR was identified as the cardinal cause of progressive deterioration of allograft function.
供体肾脏功能被认为是活体供肾(LD)肾移植后移植物存活的关键决定因素,但它对移植物功能演变的独立影响尚不清楚。本研究的目的是剖析 LD 供体肾脏功能对受者基线估算肾小球滤过率(eGFR)及其下降的相对贡献。
本研究纳入了 2007 年至 2015 年间进行的 91 例 LD 肾移植。根据同位素肾图的结果,从总 LD eGFR(eGFR-dt)计算出供体肾脏的 eGFR(eGFR-dk)。受者 eGFR(eGFR-r)在移植后 6 个月内每 6 个月测定一次,直至 36 个月,作为混合线性模型中估计基线移植物功能(截距)和 eGFR-r 斜率变化的因变量。模型除了其他潜在的混杂因素外,还分别调整了 eGFR-dk 或 eGFR-dt。
总体而言,未调整的基线 eGFR-r(6 个月)及其移植物功能的年下降率分别为 56.5mL/min/1.73m 和-0.2mL/min/1.73m。在多变量分析中,eGFR-dk 影响基线 eGFR-r(每单位增加 0.6mL/min/1.73m;P=0.02),但不影响其斜率。在 eGFR-dt 调整的模型中,LD 年龄存在边际效应(P=0.05)。两个模型都将抗体介导的排斥反应(ABMR)确定为加速移植物功能丧失的最强危险因素(eGFR-r 斜率:每年约-6mL/min/1.73m;P≤0.02)。
供体相关特征,最显著的是供体肾脏的功能和 LD 年龄,可预测基线时的 eGFR。ABMR 被确定为移植物功能进行性恶化的主要原因。