Centre for Perioperative Medicine and Critical Care Research, Imperial College Healthcare NHS Trust, London, UK.
Division of Anaesthetics, Pain Medicine and Intensive Care, Department of Surgery and Cancer, Imperial College London, London, UK.
Intensive Care Med. 2020 Apr;46(4):747-755. doi: 10.1007/s00134-019-05913-6. Epub 2020 Feb 3.
Constipation can be a significant problem in critically unwell patients, associated with detrimental outcomes. Opioids are thought to contribute to the mechanism of bowel dysfunction. We tested if methylnaltrexone, a pure peripheral mu-opioid receptor antagonist, could reverse opioid-induced constipation.
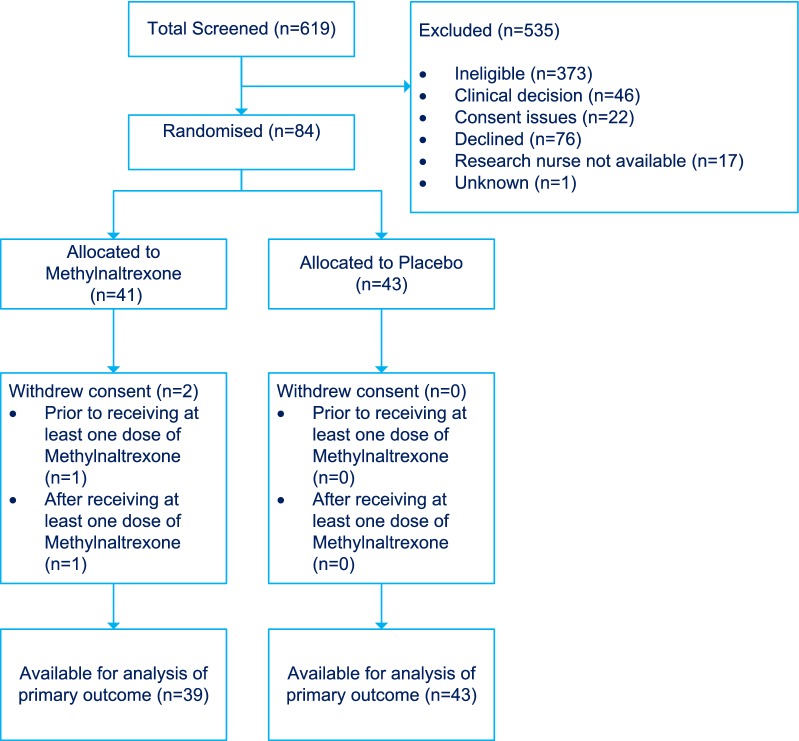
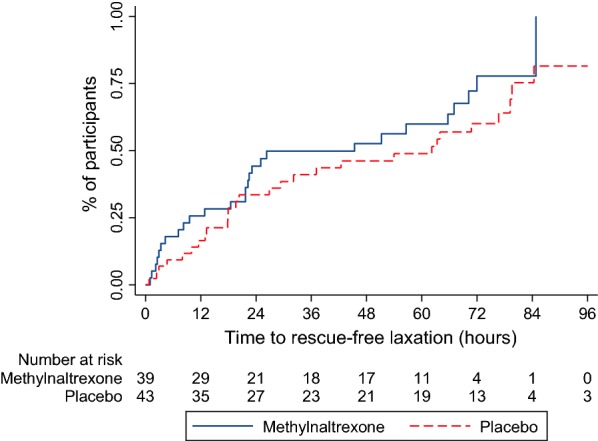
The MOTION trial is a multi-centre, double blind, randomised placebo-controlled trial to investigate whether methylnaltrexone alleviates opioid-induced constipation (OIC) in critical care patients. Eligibility criteria included adult ICU patients who were mechanically ventilated, receiving opioids and were constipated (had not opened bowels for a minimum 48 h) despite prior administration of regular laxatives as per local bowel management protocol. The primary outcome was time to significant rescue-free laxation. Secondary outcomes included gastric residual volume, tolerance of enteral feeds, requirement for rescue laxatives, requirement for prokinetics, average number of bowel movements per day, escalation of opioid dose due to antagonism/reversal of analgesia, incidence of ventilator-associated pneumonia, incidence of diarrhoea and Clostridium difficile infection and finally 28 day, ICU and hospital mortality.
A total of 84 patients were enrolled and randomized (41 to methylnaltrexone and 43 to placebo). The baseline demographic characteristics of the two groups were generally well balanced. There was no significant difference in time to rescue-free laxation between the groups (Hazard ratio 1.42, 95% CI 0.82-2.46, p = 0.22). There were no significant differences in the majority of secondary outcomes, particularly days 1-3. However, during days 4-28, there were fewer median number of bowel movements per day in the methylnaltrexone group, (p = 0.01) and a greater incidence of diarrhoea in the placebo group (p = 0.02). There was a marked difference in mortality between the groups, with ten deaths in the methylnaltrexone group and two in the placebo group during days 4-28 (p = 0.007).
We found no evidence to support the addition of methylnaltrexone to regular laxatives for the treatment of opioid-induced constipation in critically ill patients; however, the confidence interval was wide and a clinically important difference cannot be excluded.
便秘在重症患者中可能是一个严重的问题,与不良结局有关。阿片类药物被认为是导致肠道功能障碍的原因之一。我们测试了纳曲酮,一种纯外周μ-阿片受体拮抗剂,是否能逆转阿片类药物引起的便秘。
MOTION 试验是一项多中心、双盲、随机对照试验,旨在研究纳曲酮是否能缓解重症监护病房患者的阿片类药物引起的便秘(OIC)。纳入标准包括接受机械通气、接受阿片类药物且便秘(至少 48 小时未排便)的成年 ICU 患者,尽管根据当地肠道管理方案已预先给予常规泻药。主要结局是达到显著无解救性通便的时间。次要结局包括胃残留量、肠内喂养的耐受性、解救性泻药的需求、促动力药的需求、平均每天排便次数、因拮抗/逆转镇痛而增加阿片类药物剂量、呼吸机相关性肺炎的发生率、腹泻和艰难梭菌感染的发生率以及 28 天、ICU 和住院死亡率。
共纳入 84 例患者并进行随机分组(41 例纳曲酮,43 例安慰剂)。两组的基线人口统计学特征总体上均衡。两组间达到无解救性通便的时间无显著差异(风险比 1.42,95%CI 0.82-2.46,p=0.22)。大多数次要结局,特别是第 1-3 天,两组间无显著差异。然而,在第 4-28 天,纳曲酮组的平均每天排便次数更少,(p=0.01),安慰剂组的腹泻发生率更高(p=0.02)。两组间死亡率有明显差异,在第 4-28 天,纳曲酮组有 10 例死亡,安慰剂组有 2 例死亡(p=0.007)。
我们没有发现证据支持在常规泻药的基础上添加纳曲酮治疗重症患者的阿片类药物引起的便秘;然而,置信区间较宽,不能排除有临床意义的差异。