Department of Gastric Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, China.
Department of General Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, China.
J Gastrointest Surg. 2021 Feb;25(2):387-396. doi: 10.1007/s11605-020-04523-8. Epub 2020 Feb 3.
Whether the change of the pre- and postoperative systemic inflammatory response (SIR) levels will affect the prognosis of gastric cancer (GC) is unclear. We aimed to investigate the dynamic changes in the pre- and postoperative SIR and their prognostic value for GC.
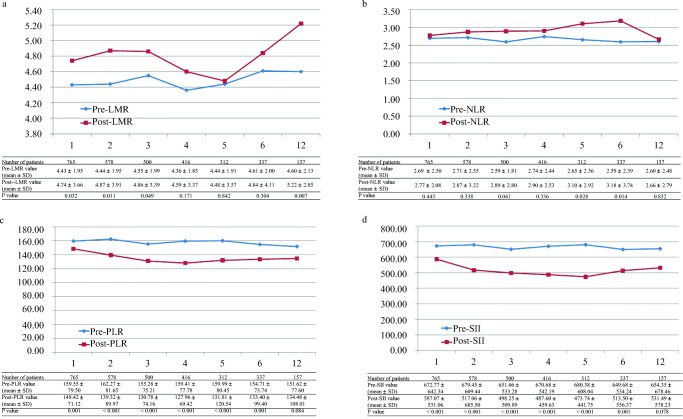
The clinicopathological data from 2257 patients who underwent radical gastrectomy between January 2009 and December 2014 at Fujian Medical University Union Hospital (FMUUH) were analyzed. Perioperative SIR changes were reported as changes in the lymphocyte-monocyte ratio (LMR), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII).
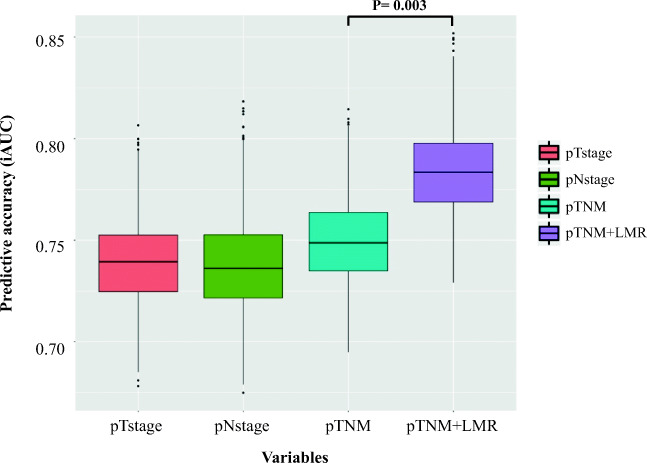
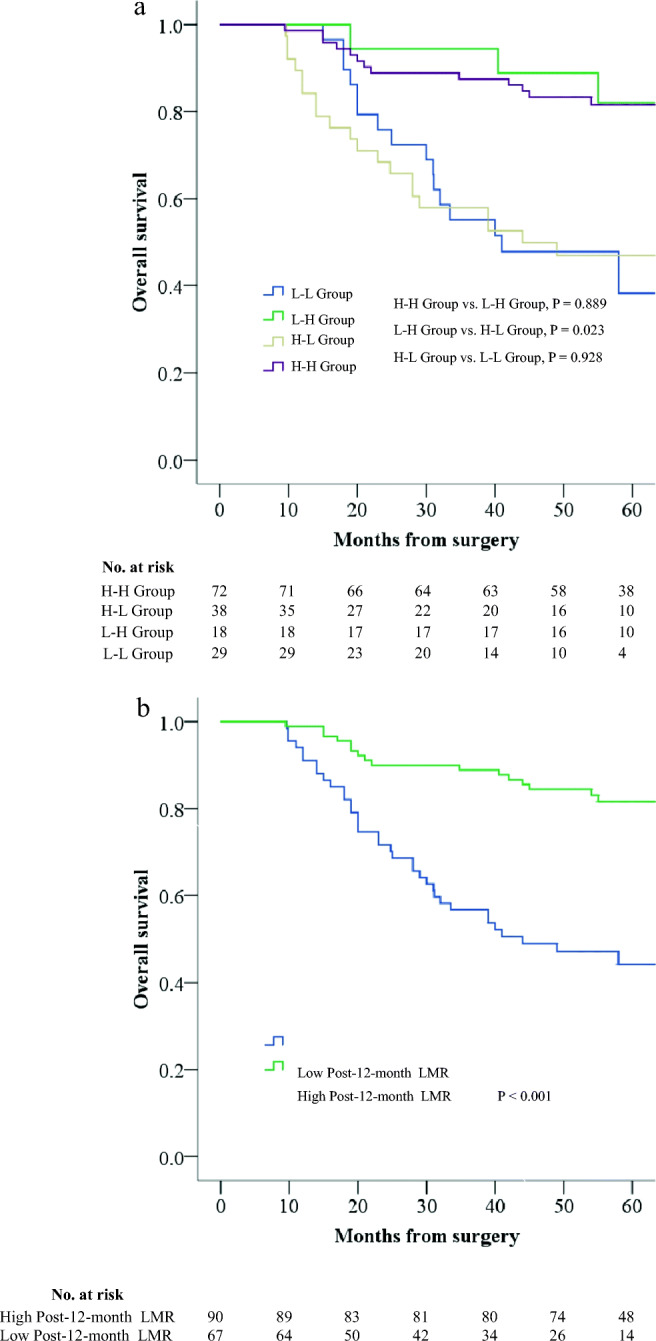
The SIR levels showed different trends from postoperative months 1 to 12. Multivariate analysis showed that preoperative (pre)-LMR was an independent predictor for the prognosis (P = 0.024). The postoperative 12-month (post-12-month) LMR predicted the 5-year overall survival (OS) rate with the highest accuracy (areas under the curve [AUC] 0.717). Patients were divided into four groups according to the optimal cutoff of the preoperative and post-12-month LMR: high pre-LMR to high postoperative (post)-LMR group, high pre-LMR to low post-LMR group, low pre-LMR to high post-LMR group, and low pre-LMR to low post-LMR group. The survival analysis showed 5-year OS rate was significantly higher in patients with high post-12-month LMR than in patients with low post-12-month LMR, regardless of pre-LMR levels (81.6% vs. 44.2%, P < 0.001). The prognostic accuracy was significantly improved by incorporating the post-12-month LMR in the tumor-node-metastasis (TNM) staging system (P = 0.003).
The remeasurement of LMR at post-12-month is helpful in predicting the long-term survival of GC.
术前和术后全身炎症反应(SIR)水平的变化是否会影响胃癌(GC)的预后尚不清楚。我们旨在研究 GC 患者术前和术后 SIR 的动态变化及其对预后的价值。
分析了 2009 年 1 月至 2014 年 12 月期间在福建医科大学附属协和医院(FMUUH)接受根治性胃切除术的 2257 例患者的临床病理资料。报告了围手术期 SIR 变化,包括淋巴细胞-单核细胞比值(LMR)、中性粒细胞-淋巴细胞比值(NLR)、血小板-淋巴细胞比值(PLR)和全身免疫炎症指数(SII)的变化。
SIR 水平在术后 1 至 12 个月呈现不同趋势。多因素分析显示,术前 LMR 是独立的预后预测因子(P=0.024)。术后 12 个月 LMR 预测 5 年总生存率(OS)的准确性最高(曲线下面积 [AUC] 0.717)。根据术前和术后 12 个月 LMR 的最佳截断值,患者被分为四组:高术前 LMR 至高术后 LMR 组、高术前 LMR 至低术后 LMR 组、低术前 LMR 至高术后 LMR 组和低术前 LMR 至低术后 LMR 组。生存分析显示,无论术前 LMR 水平如何,高术后 12 个月 LMR 组的 5 年 OS 率均显著高于低术后 12 个月 LMR 组(81.6% vs. 44.2%,P<0.001)。将术后 12 个月 LMR 纳入肿瘤-淋巴结-转移(TNM)分期系统可显著提高预后准确性(P=0.003)。
术后 12 个月时重新测量 LMR 有助于预测 GC 的长期生存。