Division of General Internal Medicine, Cedars-Sinai Medical Center, 8700 Beverly Boulevard, Los Angeles, CA 90048, USA
Department of Health Policy and Management, Harvard T H Chan School of Public Health, Boston, MA, USA.
BMJ. 2020 Feb 5;368:m40. doi: 10.1136/bmj.m40.
To examine the association between expansion of the Medicaid program under the Affordable Care Act and changes in healthcare spending among low income adults during the first four years of the policy implementation (2014-17).
Quasi-experimental difference-in-difference analysis to examine out-of-pocket spending and financial burden among low income adults after Medicaid expansions.
United States.
A nationally representative sample of individuals aged 19-64 years, with family incomes below 138% of the federal poverty level, from the 2010-17 Medical Expenditure Panel Survey.
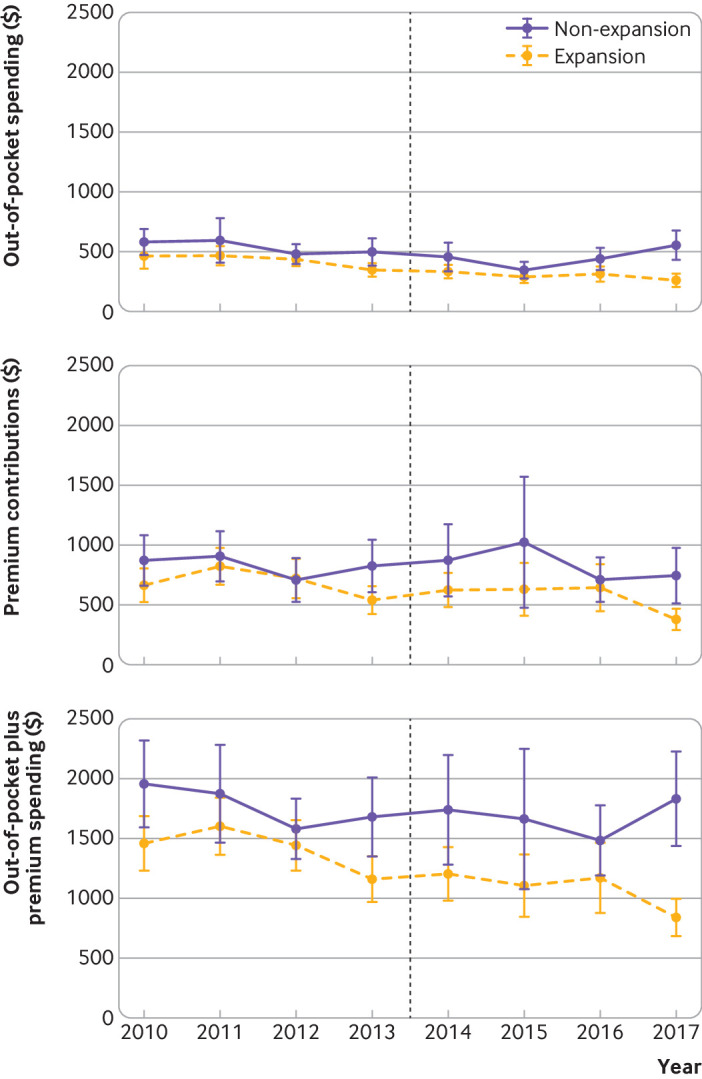
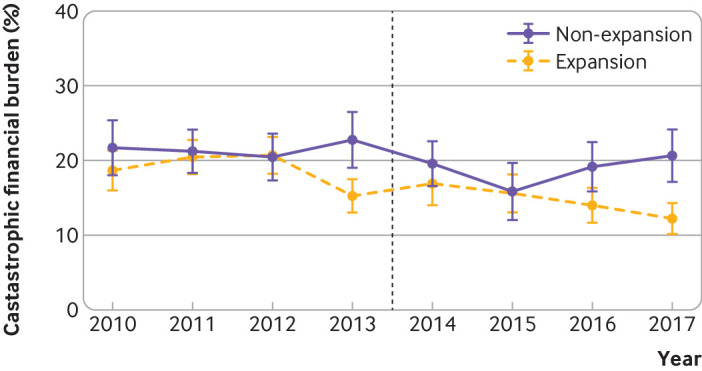
Four annual healthcare spending outcomes: out-of-pocket spending; premium contributions; out-of-pocket plus premium spending; and catastrophic financial burden (defined as out-of-pocket plus premium spending exceeding 40% of post-subsistence income). P values were adjusted for multiple comparisons.
37 819 adults were included in the study. Healthcare spending did not change in the first two years, but Medicaid expansions were associated with lower out-of-pocket spending (adjusted percentage change -28.0% (95% confidence interval -38.4% to -15.8%); adjusted absolute change -$122 (£93; €110); adjusted P<0.001), lower out-of-pocket plus premium spending (-29.0% (-40.5% to -15.3%); -$442; adjusted P<0.001), and lower probability of experiencing a catastrophic financial burden (adjusted percentage point change -4.7 (-7.9 to -1.4); adjusted P=0.01) in years three to four. No evidence was found to indicate that premium contributions changed after the Medicaid expansions.
Medicaid expansions under the Affordable Care Act were associated with lower out-of-pocket spending and a lower likelihood of catastrophic financial burden for low income adults in the third and fourth years of the act's implementation. These findings suggest that the act has been successful nationally in improving financial risk protection against medical bills among low income adults.
考察平价医疗法案(Affordable Care Act)下医疗补助计划的扩大对政策实施头四年(2014-17 年)低收入成年人医疗支出变化的影响。
对医疗补助计划扩大后低收入成年人的自付支出和经济负担进行准实验性差分差异分析。
美国。
来自 2010-17 年医疗支出面板调查的年龄在 19-64 岁之间、家庭收入低于联邦贫困水平 138%的个人,有代表性的全国性样本。
四项年度医疗保健支出结果:自付支出;保费贡献;自付加保费支出;灾难性的经济负担(定义为自付加保费支出超过生存后收入的 40%)。调整了 P 值以进行多次比较。
共纳入 37819 名成年人。前两年医疗保健支出没有变化,但医疗补助计划的扩大与较低的自付支出相关(调整后的百分比变化-28.0%(95%置信区间-38.4%至-15.8%);调整后的绝对变化-122 美元(93 英镑;110 欧元);调整后的 P<0.001),自付加保费支出也较低(-29.0%(-40.5%至-15.3%);-442 美元;调整后的 P<0.001),以及在第三至第四年经历灾难性经济负担的可能性较低(调整后的百分点变化-4.7(-7.9 至-1.4);调整后的 P=0.01)。没有证据表明保费贡献在医疗补助计划扩大后发生了变化。
平价医疗法案下的医疗补助计划扩大与该法案实施的第三和第四年低收入成年人自付支出减少和灾难性经济负担发生的可能性降低有关。这些发现表明,该法案在全国范围内成功地改善了低收入成年人对医疗账单的财务风险保护。