Sharma Bharti, Pinto Robin, Dalvi Bharat
Glenmark Cardiac Centre, Mumbai, Maharashtra, India.
Ann Pediatr Cardiol. 2020 Jan-Mar;13(1):4-10. doi: 10.4103/apc.APC_66_19. Epub 2019 Dec 4.
Device closure of secundum atrial septal defect is shown to be feasible and effective in children weighing ≤10 kg. Issues such as how large is too large, how to choose device size, does the length of the interatrial septum (IAS) matter, and need for technical modifications for successful device delivery have not been systematically addressed.
This is a retrospective study, comprising 45 patients weighing ≤10 kg, who were chosen for device closure between January 2010 and June 2018. Patient selection was done on basis of transthoracic echocardiography. Device closure was done using Amplatzer septal occluder. The device size was selected primarily based on transesophageal echocardiography (TEE)-measured defect diameter. Although IAS length was taken into consideration, adequate rim size was the key factor in deciding device closure of the defect.
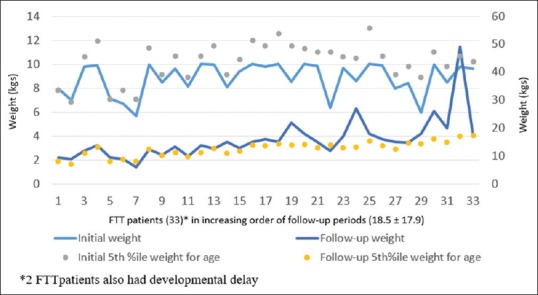
Forty-three out of 45 patients had successful device closure. The mean age and weight were 25.71 ± 8.62 months and 8.99 ± 1.24 kg, respectively. The defect measuring as large as 27 mm (14.89 ± 3.89) on TEE was closed and device as big as 28 mm was successfully deployed (16.7 ± 4.31). Regular technique of device deployment was successful in only 15 cases. In the remaining 28, one of the modified techniques was used. There was no mortality, failure of the procedure, device embolization, thromboembolism, or pericardial effusion. One patient developed moderate mitral regurgitation and two patients had transient atrioventricular block. At follow-up, all patients showed significant improvement in symptoms and growth without any complications.
Defect size as large as three times the weight in kg can be closed in small children. Devices as large as 28 mm can be deployed in these hearts provided the surrounding rims are adequate. In majority of cases, one of the modified techniques is essential for successful deployment. IAS length is not a limiting factor for deciding the size of the device used.
对于体重≤10 kg的儿童,房间隔缺损封堵术已被证明是可行且有效的。但诸如多大算过大、如何选择封堵器尺寸、房间隔(IAS)长度是否重要以及成功输送封堵器是否需要技术改进等问题尚未得到系统解决。
这是一项回顾性研究,纳入了2010年1月至2018年6月期间选择进行封堵术的45例体重≤10 kg的患者。患者选择基于经胸超声心动图。使用Amplatzer房间隔封堵器进行封堵术。封堵器尺寸主要根据经食管超声心动图(TEE)测量的缺损直径来选择。虽然考虑了IAS长度,但足够的边缘尺寸是决定封堵缺损的关键因素。
45例患者中有43例封堵成功。平均年龄和体重分别为25.71±8.62个月和8.99±1.24 kg。TEE测量最大达27 mm(14.89±3.89)的缺损被成功封堵,最大28 mm的封堵器被成功植入(16.7±4.31)。常规的封堵器植入技术仅15例成功。其余28例采用了一种改良技术。无死亡、手术失败、封堵器栓塞、血栓栓塞或心包积液发生。1例患者出现中度二尖瓣反流,2例患者发生短暂性房室传导阻滞。随访时,所有患者症状和生长均有显著改善,无任何并发症。
对于小儿患者,缺损大小可达体重(kg)的三倍仍可封堵。只要周围边缘足够,最大28 mm的封堵器可植入这些心脏。在大多数情况下,改良技术之一对于成功植入至关重要。IAS长度不是决定所用封堵器尺寸的限制因素。