Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
George Institute for Global Health, George Institute, Camperdown, Sydney, NSW, Australia.
Nephrol Dial Transplant. 2020 Feb 1;35(2):274-282. doi: 10.1093/ndt/gfz290.
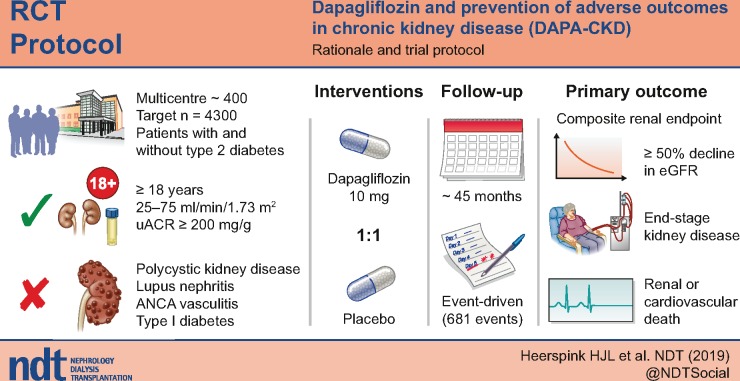
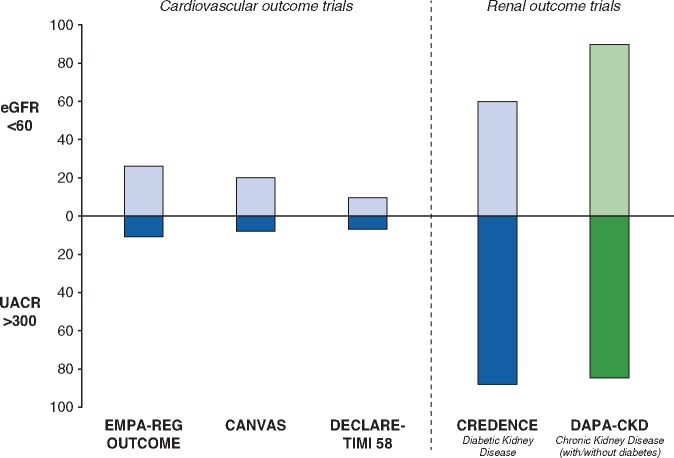
Recent cardiovascular outcome trials have shown that sodium-glucose co-transporter 2 (SGLT2) inhibitors slow the progression of chronic kidney disease (CKD) in patients with type 2 diabetes at high cardiovascular risk. Whether these benefits extend to CKD patients without type 2 diabetes or cardiovascular disease is unknown. The Dapagliflozin and Prevention of Adverse Outcomes in CKD (DAPA-CKD) trial (NCT03036150) will assess the effect of the SGLT2 inhibitor dapagliflozin on renal and cardiovascular events in a broad range of patients with CKD with and without diabetes.
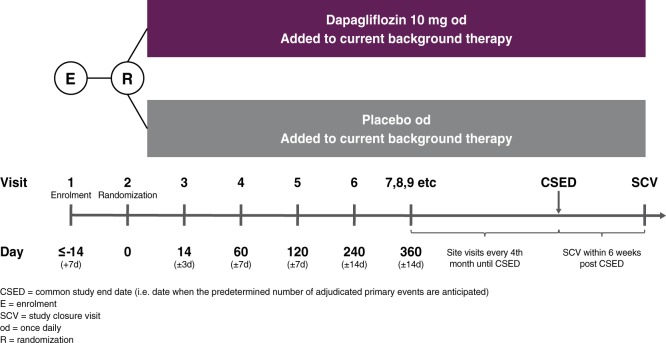
DAPA-CKD is a randomized, double-blind, placebo-controlled, trial in which ∼4300 patients with CKD Stages 2-4 and elevated urinary albumin excretion will be enrolled. The vast majority will be receiving a maximum tolerated dose of a renin-angiotensin system inhibitor at enrolment.
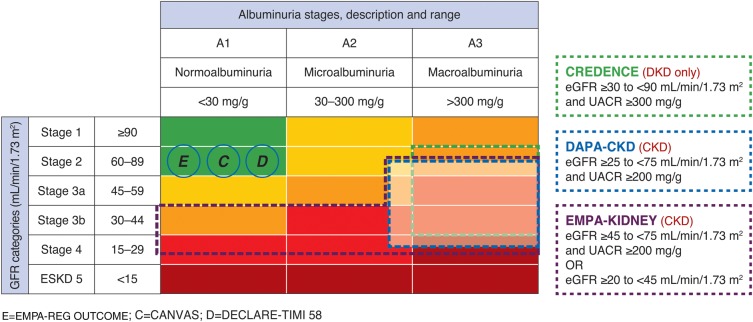
After a screening assessment, eligible patients with a urinary albumin:creatinine ratio ≥200 mg/g and estimated glomerular filtration rate (eGFR) between 25 and 75 mL/min/1.73 m2 are randomly assigned to placebo or dapagliflozin 10 mg/day. Enrolment is monitored to ensure that at least 30% of patients do not have diabetes and that no more than 10% have an eGFR >60 mL/min/1.73 m2. The primary endpoint is a composite of a sustained decline in eGFR of ≥50%, end-stage renal disease, renal death or cardiovascular death. The trial will conclude when 681 primary renal events have occurred, providing 90% power to detect a 22% relative risk reduction (α level of 0.05).
DAPA-CKD will determine whether the SGLT2 inhibitor dapagliflozin, added to guideline-recommended therapies, safely reduces the rate of renal and cardiovascular events in patients across multiple CKD stages with and without diabetes.
最近的心血管结局试验表明,钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂可减缓高心血管风险的 2 型糖尿病患者慢性肾脏病(CKD)的进展。这些益处是否扩展到没有 2 型糖尿病或心血管疾病的 CKD 患者尚不清楚。达格列净和预防 CKD 不良结局(DAPA-CKD)试验(NCT03036150)将评估 SGLT2 抑制剂达格列净对广泛的 CKD 患者(无论是否患有糖尿病)的肾脏和心血管事件的影响。
DAPA-CKD 是一项随机、双盲、安慰剂对照试验,约 4300 名 CKD 2-4 期和尿白蛋白排泄量升高的患者将入组。绝大多数患者在入组时将接受最大耐受剂量的肾素-血管紧张素系统抑制剂。
在筛选评估后,符合条件的患者尿白蛋白:肌酐比≥200mg/g 和估算肾小球滤过率(eGFR)在 25 至 75mL/min/1.73m2 之间,随机分配至安慰剂或达格列净 10mg/天。登记处受到监测,以确保至少 30%的患者没有糖尿病,并且不超过 10%的患者 eGFR>60mL/min/1.73m2。主要终点是 eGFR 持续下降≥50%、终末期肾病、肾脏死亡或心血管死亡的复合终点。当发生 681 例主要肾脏事件时,试验将结束,提供 90%的效能以检测 22%的相对风险降低(α水平为 0.05)。
DAPA-CKD 将确定 SGLT2 抑制剂达格列净是否在多个 CKD 阶段和有无糖尿病的患者中,与指南推荐的治疗方法联合使用,安全地降低肾脏和心血管事件的发生率。