Department of Medicine, Division of Cardiovascular Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA; and.
InCarda Therapeutics, Newark, CA.
J Cardiovasc Pharmacol. 2020 Apr;75(4):276-283. doi: 10.1097/FJC.0000000000000804.
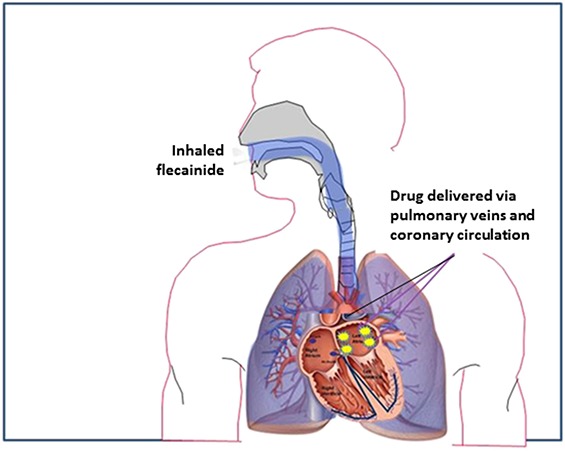
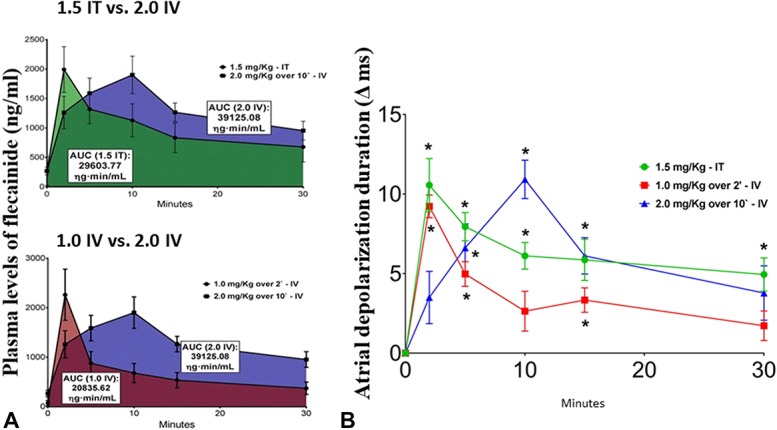
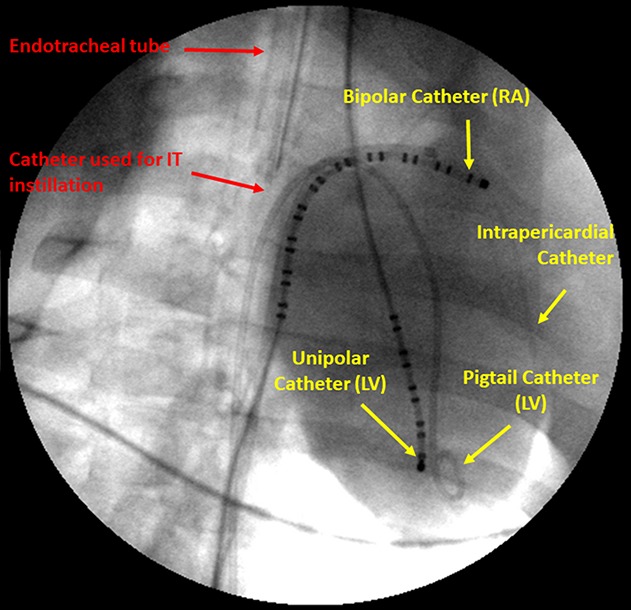
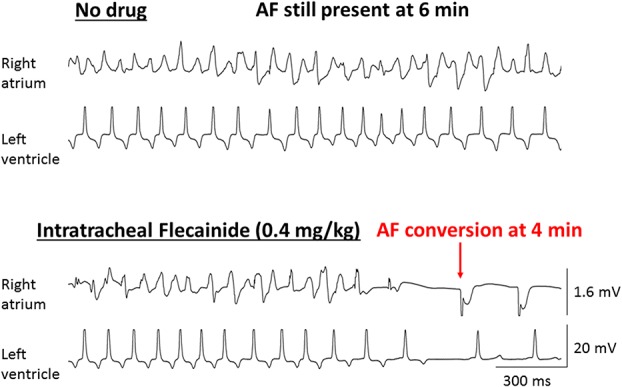
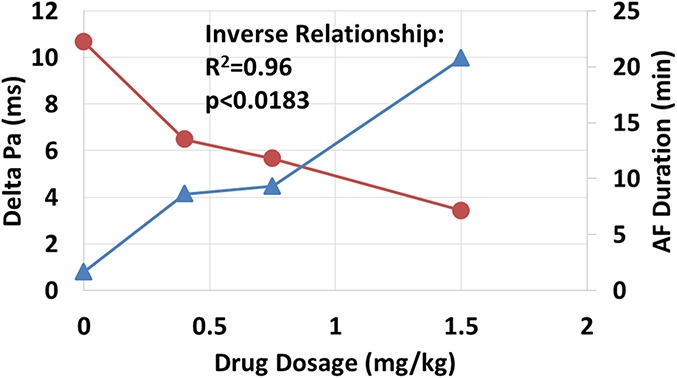
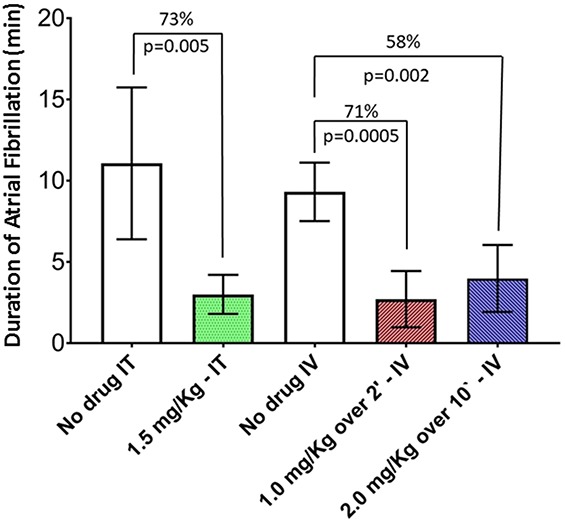
Pharmacologic management of atrial fibrillation (AF) is a pressing problem. This arrhythmia afflicts >5 million individuals in the United States and prevalence is estimated to rise to 12 million by 2050. Although the pill-in-the-pocket regimen for self-administered AF cardioversion introduced over a decade ago has proven useful, significant drawbacks exist. Among these are the relatively long latency of effects in the range of hours along with potential for hypotension and other adverse effects. This experience prompted development of a new strategy for increasing plasma concentrations of antiarrhythmic drugs rapidly and for a limited time, namely, pulmonary delivery. In preclinical studies in Yorkshire pigs, intratracheal administration of flecainide was shown to cause a rapid, reproducible increase in plasma drug levels. Moreover, pulmonary delivery of flecainide converted AF to normal sinus rhythm by prolonging atrial depolarization, which slows intra-atrial conduction and seems to be directly correlated with efficacy in converting AF. The rapid rise in plasma flecainide levels optimizes its anti-AF effects while minimizing adverse influences on ventricular depolarization and contractility. A more concentrated and soluble formulation of flecainide using a novel cyclodextrin complex excipient reduced net drug delivery for AF conversion when compared to the acetate formulation. Inhalation of the beta-adrenergic blocking agent metoprolol slows ventricular rate and can also terminate AF. In human subjects, oral inhalation of flecainide acetate with a hand-held, breath-actuated nebulizer results in signature prolongation of the QRS complex without serious adverse events. Thus, pulmonary delivery is a promising advance in pharmacologic approach to management of AF.
心房颤动(AF)的药物治疗是一个紧迫的问题。这种心律失常在美国影响超过 500 万人,预计到 2050 年患病率将上升到 1200 万。尽管十多年前推出的用于自我管理 AF 电复律的口袋药丸方案已被证明有用,但仍存在一些明显的缺陷。其中包括作用的潜伏期相对较长,范围在数小时内,以及可能出现低血压和其他不良反应。这一经验促使人们开发了一种新策略,即通过肺部输送来快速且有限时间地增加抗心律失常药物的血浆浓度。在约克郡猪的临床前研究中,经气管内给予氟卡尼被证明可迅速、可重复地增加血浆药物水平。此外,通过延长心房去极化,肺输送氟卡尼可将 AF 转为正常窦性节律,从而减慢房内传导,这似乎与将 AF 转为正常窦性节律的疗效直接相关。血浆氟卡尼水平的快速升高优化了其抗 AF 作用,同时最大限度地减少了对心室去极化和收缩力的不良影响。使用新型环糊精复合赋形剂的氟卡尼更浓缩和更易溶的配方与醋酸盐配方相比,用于 AF 转换时,药物总输送量减少。β-肾上腺素能阻滞剂美托洛尔的吸入可降低心室率,也可终止 AF。在人体受试者中,使用手持式、呼吸触发的雾化器口服吸入氟卡尼醋酸盐可导致 QRS 复合体明显延长,而无严重不良事件。因此,肺部输送是 AF 药物治疗方法的一个有前途的进展。