Wittenstein Jakob, Scharffenberg Martin, Braune Anja, Huhle Robert, Bluth Thomas, Herzog Moritz, Güldner Andreas, Ball Lorenzo, Simonassi Francesca, Zeidler-Rentzsch Ines, Vidal Melo Marcos F, Koch Thea, Rocco Patricia R M, Pelosi Paolo, Kotzerke Jörg, Gama de Abreu Marcelo, Kiss Thomas
Department of Anesthesiology and Intensive Care Medicine, Pulmonary Engineering Group, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
Department of Anesthesiology and Intensive Care Medicine, Pulmonary Engineering Group, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany; Department of Nuclear Medicine, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
Br J Anaesth. 2020 Apr;124(4):430-439. doi: 10.1016/j.bja.2019.12.040. Epub 2020 Feb 6.
Mechanical ventilation with variable tidal volumes (V) may improve lung function and reduce ventilator-induced lung injury in experimental acute respiratory distress syndrome (ARDS). However, previous investigations were limited to less than 6 h, and control groups did not follow clinical standards. We hypothesised that 24 h of mechanical ventilation with variable V reduces pulmonary inflammation (as reflected by neutrophil infiltration), compared with standard protective, nonvariable ventilation.
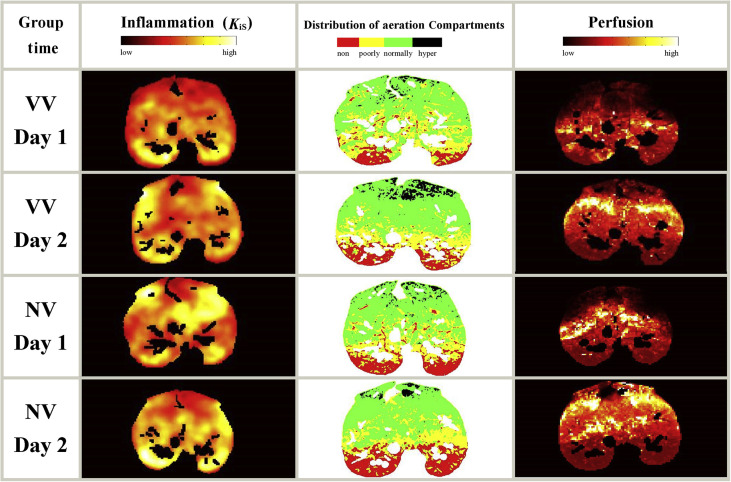
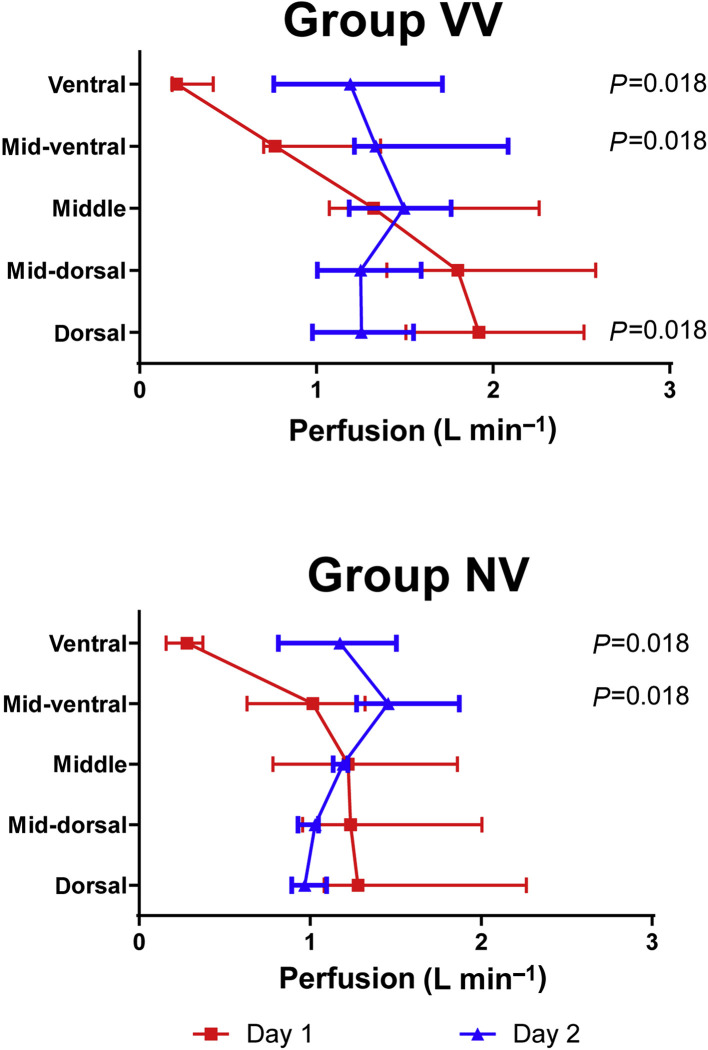
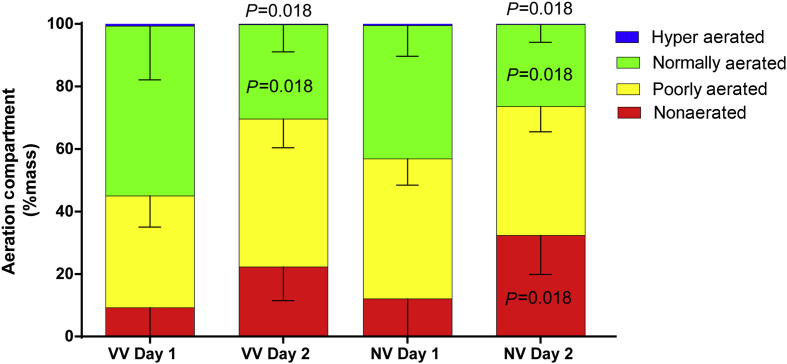
Experimental ARDS was induced in 14 anaesthetised pigs with saline lung lavage followed by injurious mechanical ventilation. Pigs (n=7 per group) were randomly assigned to using variable V or nonvariable V modes of mechanical ventilation for 24 h. In both groups, ventilator settings including positive end-expiratory pressure and oxygen inspiratory fraction were adjusted according to the ARDS Network protocol. Pulmonary inflammation (primary endpoint) and perfusion were assessed by positron emission tomography using 2-deoxy-2-[F]fluoro-d-glucose and Gallium (Ga)-labelled microspheres, respectively. Gas exchange, respiratory mechanics, and haemodynamics were quantified. Lung aeration was determined using CT.
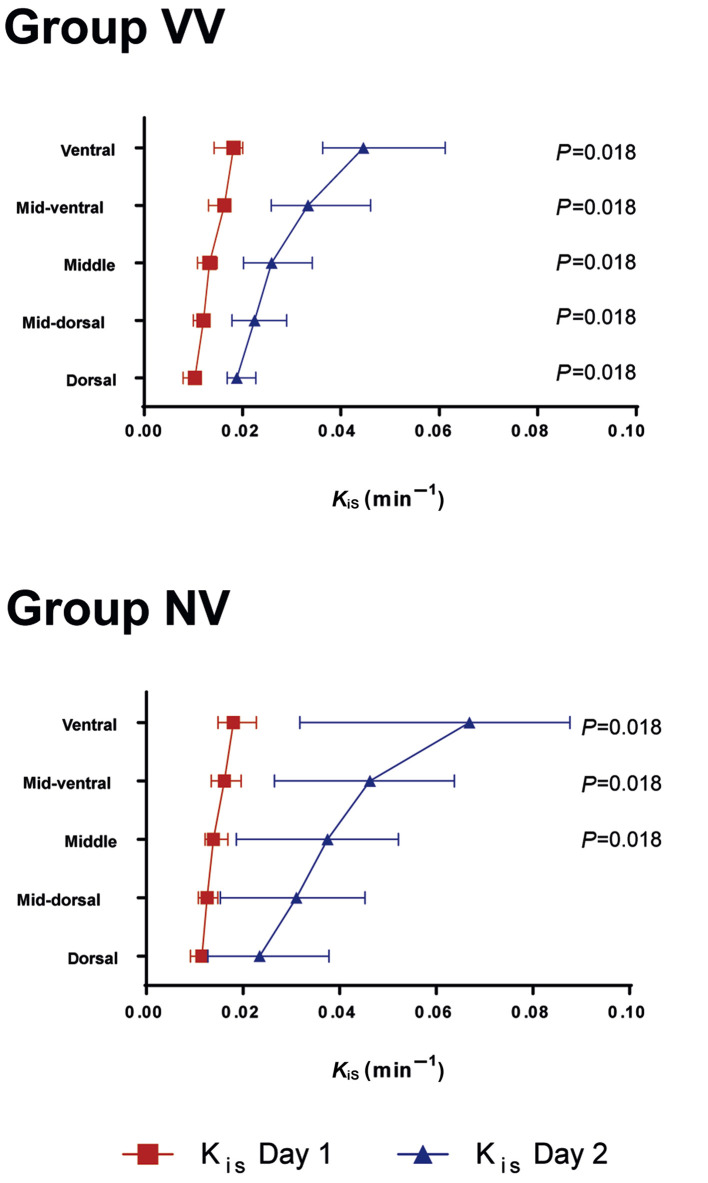
The specific global uptake rate of F-FDG increased to a similar extent regardless of mode of mechanical ventilation (median uptake for variable V=0.016 min [inter-quartile range, 0.012-0.029] compared with median uptake for nonvariable V=0.037 min [0.008-0.053]; P=0.406). Gas exchange, respiratory mechanics, haemodynamics, and lung aeration and perfusion were similar in both variable and nonvariable V ventilatory modes.
In a porcine model of ARDS, 24 h of mechanical ventilation with variable V did not attenuate pulmonary inflammation compared with standard protective mechanical ventilation with nonvariable V.
在实验性急性呼吸窘迫综合征(ARDS)中,采用可变潮气量(V)进行机械通气可能改善肺功能并减少呼吸机诱发的肺损伤。然而,先前的研究限于6小时以内,且对照组未遵循临床标准。我们假设,与标准的保护性、固定通气相比,采用可变V进行24小时机械通气可减轻肺部炎症(以中性粒细胞浸润为指标)。
对14只麻醉猪进行生理盐水肺灌洗,随后进行损伤性机械通气,诱导实验性ARDS。将猪(每组n = 7)随机分配,分别采用可变V或固定V模式进行机械通气24小时。两组均根据ARDS网络方案调整呼吸机设置,包括呼气末正压和吸气氧分数。分别采用2-脱氧-2-[F]氟-D-葡萄糖和镓(Ga)标记的微球,通过正电子发射断层扫描评估肺部炎症(主要终点)和灌注。对气体交换、呼吸力学和血流动力学进行量化。采用CT测定肺通气情况。
无论机械通气模式如何,F-FDG的特定全身摄取率均以相似幅度增加(可变V组的摄取中位数 = 0.016分钟[四分位间距,0.012 - 0.029],固定V组的摄取中位数 = 0.037分钟[0.008 - 0.053];P = 0.406)。可变V和固定V通气模式下的气体交换、呼吸力学、血流动力学以及肺通气和灌注情况相似。
在ARDS猪模型中,与采用固定V的标准保护性机械通气相比,采用可变V进行24小时机械通气并未减轻肺部炎症。