Division of Nephrology.
Department of Medicine.
Clin J Am Soc Nephrol. 2020 Feb 7;15(2):174-181. doi: 10.2215/CJN.05050419.
We conducted a pilot, pragmatic, cluster-randomized trial to evaluate feasibility and preliminary effectiveness of screening for CKD using a triple-marker approach (creatinine, cystatin C, and albumin/creatinine ratio), followed by education and guidance, to improve care of hypertensive veterans in primary care. We used the electronic health record for identification, enrollment, intervention delivery, and outcome ascertainment.
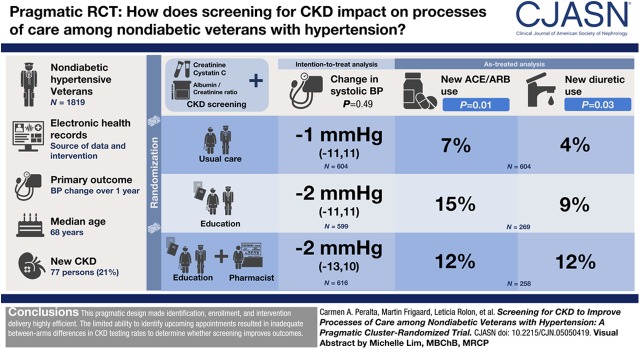
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We randomized 1819 veterans without diabetes but with hypertension (41 clusters) into three arms: () CKD screening followed by patient and provider education; () screening, education, plus pharmacist comanagement; or () usual care. The primary clinical outcome was BP change over 1 year. Implementation and process measures included proportion screened; CKD detection rate; and total and new use of renin-angiotensin system inhibitors, nonsteroidal anti-inflammatory drugs, and diuretics.
Median age was 68 years, 55% were white, 1658 (91%) had a prior creatinine measure, but only 172 (9%) had prior urine albumin/creatinine ratio, and 83 (5%) had a prior cystatin C measure. Among those in the intervention, 527 of 1215 (43%) were identified with upcoming appointments to have CKD screening. Of these, 367 (69%) completed testing. Among those tested, 77 (21%) persons had newly diagnosed CKD. After 1 year, change in systolic BP was -1 mm Hg (interquartile range, -11 to 11) in usual care, -2 mm Hg (-11 to 11) in the screen-educate arm, and -2 mm Hg (-13 to 10) in the screen-educate plus pharmacist arm; =0.49. There were no significant differences in secondary outcomes in intention-to-treat analyses. In as-treated analyses, higher proportions of participants in the intervention arms initiated a renin-angiotensin system inhibitor (15% and 12% versus 7% in usual care, =0.01) or diuretic (9% and 12% versus 4%, =0.03).
The pragmatic design made identification, enrollment, and intervention delivery highly efficient. The limited ability to identify appointments resulted in inadequate between-arm differences in CKD testing rates to determine whether screening improves clinical outcomes.
我们进行了一项前瞻性、实用、集群随机试验,以评估使用三重标志物(肌酐、胱抑素 C 和白蛋白/肌酐比)筛查 CKD 的可行性和初步疗效,然后进行教育和指导,以改善初级保健中高血压退伍军人的护理。我们使用电子健康记录进行识别、入组、干预交付和结果确定。
设计、设置、参与者和测量:我们将 1819 名无糖尿病但患有高血压的退伍军人(41 个集群)随机分为三组:() CKD 筛查后进行患者和提供者教育;() 筛查、教育、加上药剂师共同管理;或() 常规护理。主要临床结果是 1 年内血压变化。实施和过程措施包括筛查比例;CKD 检出率;以及肾素-血管紧张素系统抑制剂、非甾体抗炎药和利尿剂的总使用量和新用量。
中位年龄为 68 岁,55%为白人,1658 名(91%)有既往肌酐测量值,但只有 172 名(9%)有既往尿白蛋白/肌酐比值,83 名(5%)有既往胱抑素 C 测量值。在干预组中,1215 名中有 527 名(43%)被确定即将进行 CKD 筛查。其中,367 名(69%)完成了检测。在接受检测的人群中,77 名(21%)人被新诊断为 CKD。1 年后,常规护理组收缩压变化为-1mmHg(四分位间距,-11 至 11),筛查-教育组为-2mmHg(-11 至 11),筛查-教育加药剂师组为-2mmHg(-13 至 10);=0.49。意向治疗分析中无次要结局差异。在实际治疗分析中,干预组中更多的参与者开始使用肾素-血管紧张素系统抑制剂(15%和 12%,而常规护理组为 7%,=0.01)或利尿剂(9%和 12%,而常规护理组为 4%,=0.03)。
实用设计使识别、入组和干预交付非常高效。确定预约的能力有限,导致 CKD 检测率在组间差异不足,无法确定筛查是否改善临床结局。