Department of Diabetes, Central Clinical School, Monash University, Melbourne, Victoria, Australia.
Dallas Diabetes Research Center at Medical City, Dallas, Texas.
Diabetes Obes Metab. 2020 Jul;22(7):1062-1073. doi: 10.1111/dom.13995. Epub 2020 Feb 27.
In CARMELINA®, linagliptin demonstrated cardiovascular and renal safety in patients with type 2 diabetes (T2D) with high renal and cardiovascular disease (CVD) risk. We investigated safety and efficacy of this dipeptidyl peptidase-4 inhibitor in older participants.
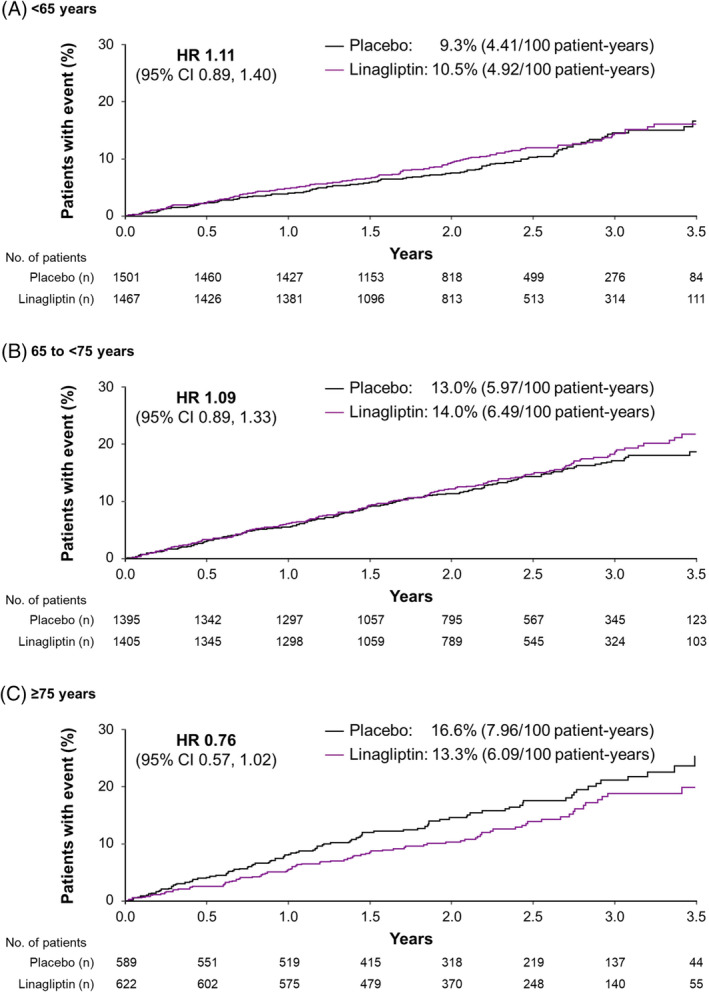
Subjects aged ≥18 years with T2D and established CVD with urinary albumin-to-creatinine ratio (UACR) >30 mg/g, and/or prevalent kidney disease, were randomized to linagliptin or placebo added to usual care. The primary endpoint (time to first occurrence of 3P-MACE: cardiovascular death, non-fatal myocardial infarction or non-fatal stroke) and other outcomes were evaluated across age groups <65 (n = 2968), 65 to <75 (n = 2800) and ≥75 years (n = 1211).
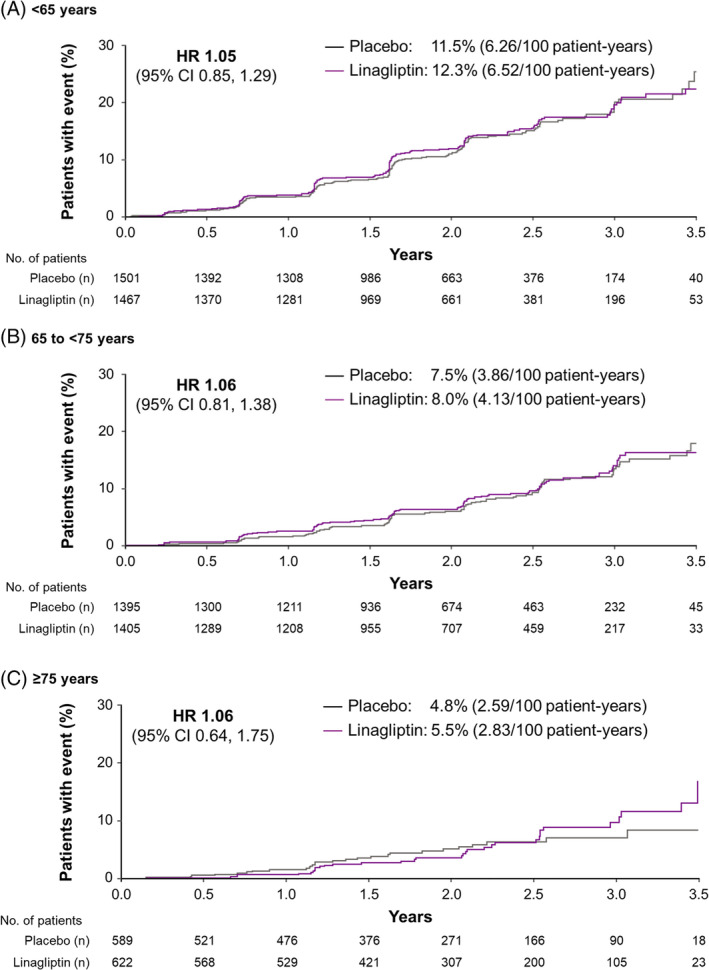
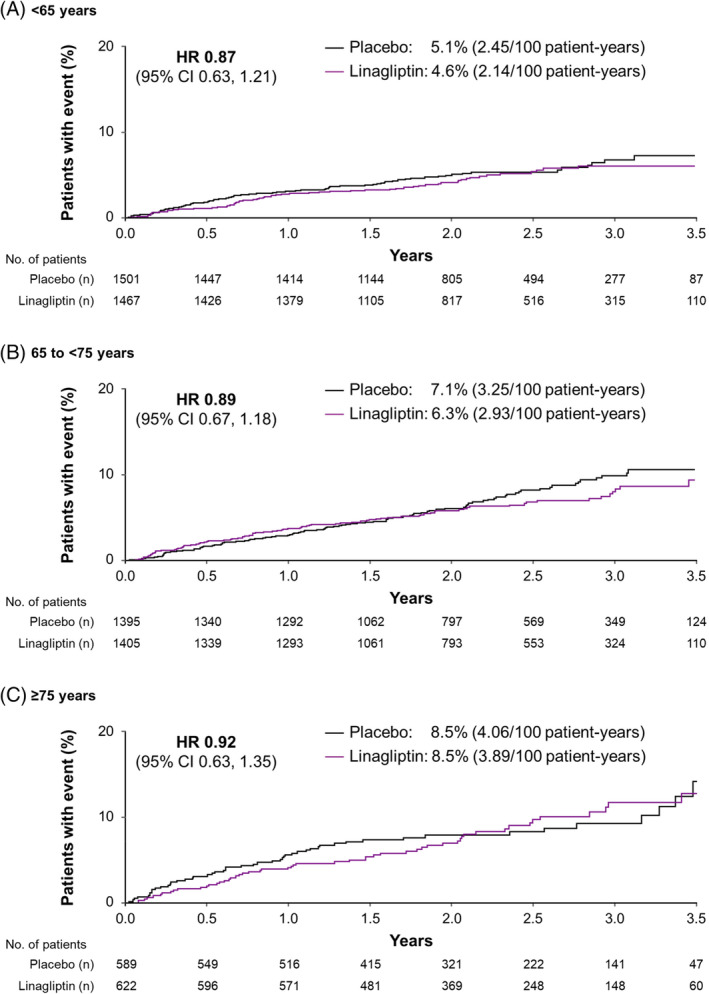
Mean age was 65.9 years (17.4% and 5.9% aged ≥75 and 80, respectively) and median follow-up was 2.2 years. The hazard ratio (HR) for 3P-MACE with linagliptin versus placebo was 1.02 [95% confidence interval (CI) 0.89, 1.17] with no significant interaction between age and treatment effect (P = 0.0937). HRs for participants aged <65, 65 to <75 and ≥75 years were 1.11 (95% CI 0.89, 1.40), 1.09 (0.89, 1.33) and 0.76 (0.57, 1.02), respectively. Linagliptin did not increase the risk of adverse kidney outcomes or hospitalization for heart failure across age groups. The incidence of adverse events, including hypoglycaemia, increased with age but was similar with linagliptin and placebo despite glycated haemoglobin A1c reduction with linagliptin.
Linagliptin did not increase risk for cardiovascular events or hypoglycaemia and kidney function remained stable in older people with T2D and established CVD with albuminuria and/or kidney disease.
在 CARMELINA®研究中,利格列汀在伴有高肾脏和心血管疾病(CVD)风险的 2 型糖尿病(T2D)患者中表现出心血管和肾脏安全性。我们研究了这种二肽基肽酶-4 抑制剂在老年患者中的安全性和疗效。
年龄≥18 岁、患有 T2D 且尿白蛋白与肌酐比值(UACR)>30mg/g,或已有肾脏疾病的患者,被随机分配至接受利格列汀或安慰剂联合常规治疗。主要终点(3P-MACE 的首次发生时间:心血管死亡、非致死性心肌梗死或非致死性卒中)和其他结局在年龄<65 岁(n=2968)、65-<75 岁(n=2800)和≥75 岁(n=1211)的患者中进行评估。
平均年龄为 65.9 岁(分别有 17.4%和 5.9%的患者年龄≥75 岁和 80 岁),中位随访时间为 2.2 年。与安慰剂相比,利格列汀组 3P-MACE 的风险比(HR)为 1.02[95%置信区间(CI)0.89,1.17],且年龄与治疗效果之间无显著交互作用(P=0.0937)。年龄<65 岁、65-<75 岁和≥75 岁的患者 HR 分别为 1.11(95%CI 0.89,1.40)、1.09(0.89,1.33)和 0.76(0.57,1.02)。利格列汀并未增加各年龄组不良肾脏结局或心力衰竭住院的风险。不良事件(包括低血糖)的发生率随年龄增长而增加,但由于利格列汀降低糖化血红蛋白 A1c,因此与安慰剂相比,其在利格列汀和安慰剂中的发生率相似。
在伴有蛋白尿和/或肾脏疾病的伴有 CVD 的老年 T2D 患者中,利格列汀不会增加心血管事件或低血糖的风险,且肾功能保持稳定。