Department of Pathology, Northwestern University, Chicago, IL, 60630, USA.
Department of Neurosurrgery, Northwestern University, Chicago, IL, 60630, USA.
Acta Neuropathol Commun. 2020 Feb 12;8(1):15. doi: 10.1186/s40478-020-0892-2.
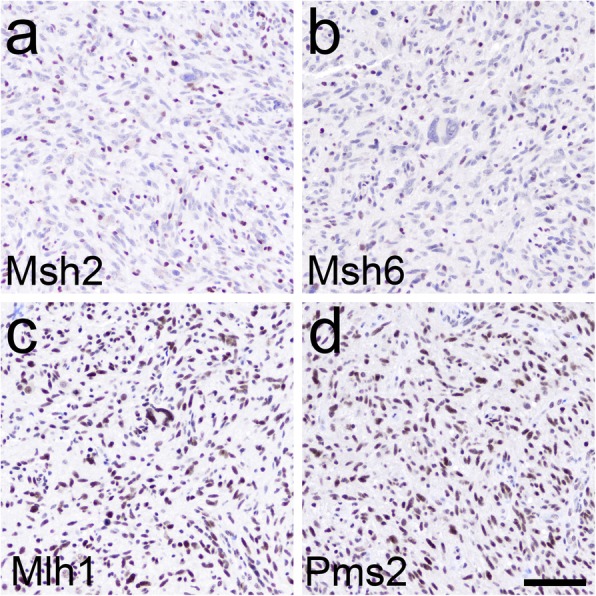
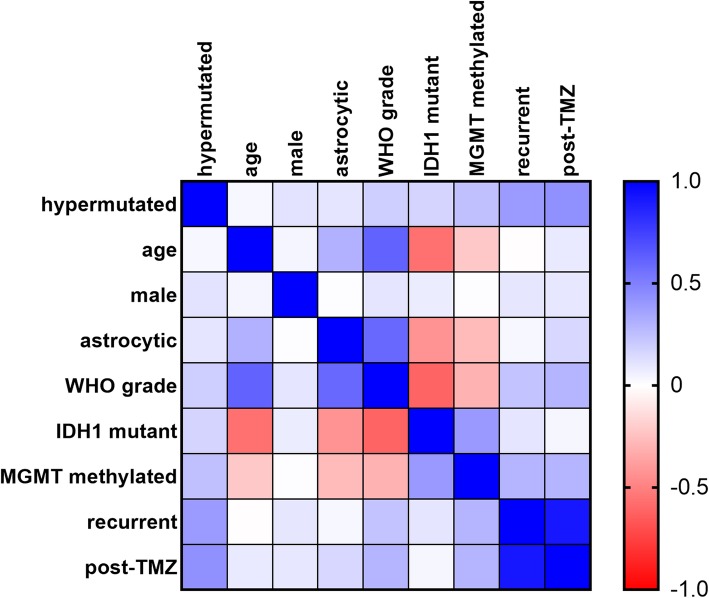
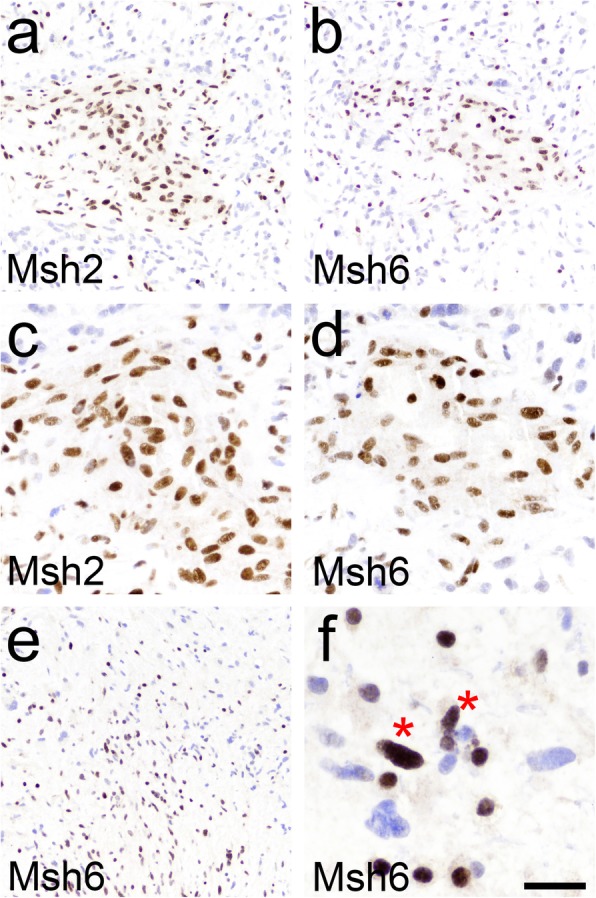
A subset of gliomas has DNA repair defects that lead to hypermutated genomes. While such tumors are resistant to alkylating chemotherapies, they may also express more mutant neoantigens on their cell surfaces, and thus be more responsive to immunotherapies. A fast, inexpensive method of screening for hypermutated gliomas would therefore be of great clinical value. Since immunohistochemistry (IHC) for the DNA mismatch repair (MMR) proteins Msh2, Msh6, Mlh1, and Pms2 is already used to screen for hypermutated colorectal cancers, we sought to determine whether that panel might have similar utility in gliomas. MMR IHC was scored in 100 WHO grade I-IV gliomas (from 96 patients) with known tumor mutation burden (TMB), while blinded to TMB data. Cases included 70 grade IV GBMs, 13 grade III astrocytomas, 4 grade II astrocytomas (3 diffuse astrocytomas and 1 pleomorphic xanthoastrocytoma), 1 grade I pilocytic astrocytoma, 2 grade III oligodendrogliomas, 7 grade II oligodendrogliomas, and 3 grade I glioneuronal tumors. Eight of 100 tumors showed loss of one or more MMR proteins by IHC, and all 8 were hypermutated. Among the remaining 92 gliomas with intact MMR IHC, only one was hypermutated; that tumor had an inactivating mutation in another DNA repair gene, ATM. Overall accuracy, sensitivity, and specificity for DNA MMR IHC compared to the gold standard of TMB were 99, 89, and 100%, respectively. The strongest correlates with hypermutation were prior TMZ treatment, MGMT promoter methylation, and IDH1 mutation. Among the 8 MMR-deficient hypermutated gliomas, 4 (50%) contained both MMR-lost and MMR-retained tumor cells. Together, these data suggest that MMR IHC could be a viable front-line screening test for gliomas in which immunotherapy is being considered. They also suggest that not all cells in a hypermutated glioma may actually be MMR-deficient, a finding that might need to be considered when treating such tumors with immunotherapies.
一部分神经胶质瘤存在 DNA 修复缺陷,导致基因组发生超突变。尽管此类肿瘤对烷化剂化疗具有抗性,但它们的细胞表面可能也会表达更多的突变新抗原,因此对免疫疗法更敏感。因此,一种快速、廉价的筛选超突变神经胶质瘤的方法将具有重要的临床价值。由于免疫组织化学(IHC)检测 DNA 错配修复(MMR)蛋白 Msh2、Msh6、Mlh1 和 Pms2 已用于筛选超突变结直肠癌,我们试图确定该面板在神经胶质瘤中是否具有类似的作用。对 100 例已知肿瘤突变负担(TMB)的 WHO 分级 I-IV 神经胶质瘤(来自 96 例患者)进行了 MMR IHC 评分,而评分时对 TMB 数据不知情。这些病例包括 70 例 IV 级胶质母细胞瘤、13 例 III 级星形细胞瘤、4 例 II 级星形细胞瘤(3 例弥漫性星形细胞瘤和 1 例多形性黄色星形细胞瘤)、1 例 I 级毛细胞星形细胞瘤、2 例 III 级少突胶质细胞瘤、7 例 II 级少突胶质细胞瘤和 3 例 I 级神经胶质神经元肿瘤。通过 IHC 显示 100 例肿瘤中有 8 例失去 1 种或多种 MMR 蛋白,且这 8 例均为超突变。在其余 92 例 MMR IHC 完整的神经胶质瘤中,只有 1 例为超突变;该肿瘤存在另一种 DNA 修复基因 ATM 的失活突变。与 TMB 这一金标准相比,DNA MMR IHC 的总体准确性、敏感性和特异性分别为 99%、89%和 100%。与超突变最密切相关的因素是先前的 TMZ 治疗、MGMT 启动子甲基化和 IDH1 突变。在 8 例 MMR 缺陷的超突变神经胶质瘤中,有 4 例(50%)同时存在 MMR 缺失和 MMR 保留的肿瘤细胞。总的来说,这些数据表明,MMR IHC 可能是一种可行的一线筛选测试,可用于考虑免疫治疗的神经胶质瘤。它们还表明,并非所有超突变神经胶质瘤的细胞实际上都存在 MMR 缺陷,在使用免疫疗法治疗此类肿瘤时,可能需要考虑这一发现。