Wang Tongtong, Patel Shrita M, Hickman Anne, Liu Xinyue, Jones Philip LStJ, Gantz Ira, Koro Carol E
Department of Pharmacoepidemiology, Merck & Co., Inc., Kenilworth, NJ, USA.
Department of Clinical Safety and Risk Management, Merck & Co., Inc., Kenilworth, NJ, USA.
Diabetes Ther. 2020 Mar;11(3):711-723. doi: 10.1007/s13300-020-00771-8. Epub 2020 Feb 12.
Based on post-marketing surveillance, concern has been raised that sodium-glucose cotransporter 2 inhibitors (SGLT2i) may increase the risk of necrotizing fasciitis of the perineum (Fournier's gangrene, FG). As a result of the low incidence of FG, data from clinical trials may be insufficient to robustly assess this issue because of the relatively limited numbers of participants. Real-world evidence may help clarify the association between SGLT2i and FG in the type 2 diabetes (T2D) population.
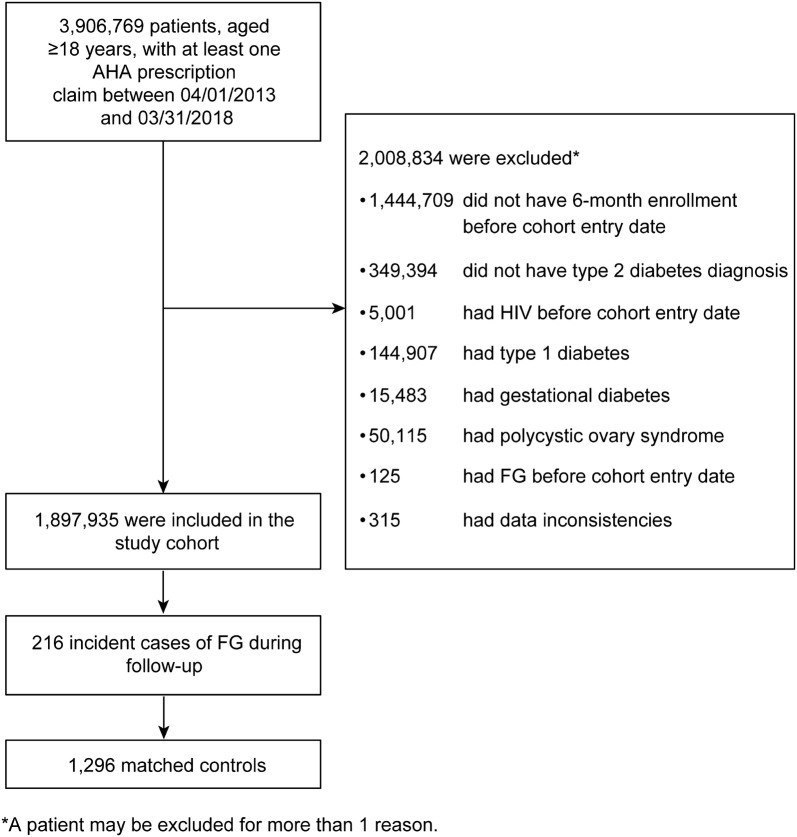
A nested case-control study was performed using Truven Health MarketScan™ databases. Each patient with T2D hospitalized for FG between 1 April 2013 (when the first SGLT2i was available) and 31 March 2018 (latest available data) was matched (on the basis of sex, age, and cohort entry date) with six controls from the same cohort. The adjusted odds ratio (OR) of hospitalization for FG was estimated for patients receiving SGLT2i compared with those receiving two or more non-SGLT2i antihyperglycemic agents (AHAs) or insulin alone using conditional logistic regression.
The cohort included 1,897,935 patients, with 216 hospitalized for FG (incidence rate, 5.2 events per 100,000 person-years). Patients with FG ranged from 23 to 79 years of age; 201 (93.1%) were men. Among the 216 FG cases, 9 (4.2%) were current SGLT2i users; among the 1296 matched controls, 100 (7.7%) were current SGLT2i users. Approximately 93% of SGLT2i were used in combination. The adjusted OR of FG in patients treated with SGLT2i compared with patients treated with two or more non-SGLT2i AHAs or insulin alone was 0.55 [95% CI 0.25-1.18].
The study did not find that treatment with SGLT2i, as compared with treatment with two or more non-SGLT2i AHAs or insulin alone, was statistically significantly associated with an increased risk of hospitalization for FG. Additional studies are needed to corroborate the findings.
基于上市后监测,有人担心钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)可能会增加会阴坏死性筋膜炎(福尼埃坏疽,FG)的风险。由于FG发病率较低,临床试验数据可能不足以有力地评估这一问题,因为参与者数量相对有限。真实世界证据可能有助于阐明SGLT2i与2型糖尿病(T2D)人群中FG之间的关联。
使用Truven Health MarketScan™数据库进行了一项巢式病例对照研究。2013年4月1日(首个SGLT2i上市)至2018年3月31日(最新可用数据)期间因FG住院的每例T2D患者,与来自同一队列的6名对照(根据性别、年龄和队列入组日期)进行匹配。使用条件逻辑回归,估计接受SGLT2i治疗的患者与接受两种或更多种非SGLT2i降糖药物(AHA)或仅接受胰岛素治疗的患者相比,因FG住院的调整优势比(OR)。
该队列包括1,897,935例患者,其中216例因FG住院(发病率为每100,000人年5.2例)。FG患者年龄在23至79岁之间;201例(93.1%)为男性。在216例FG病例中,9例(4.2%)为当前SGLT2i使用者;在1296例匹配对照中,100例(7.7%)为当前SGLT2i使用者。约93%的SGLT2i为联合使用。与接受两种或更多种非SGLT2i AHA或仅接受胰岛素治疗的患者相比,接受SGLT2i治疗的患者发生FG的调整OR为0.55 [95%CI 0.25-1.18]。
该研究未发现与接受两种或更多种非SGLT2i AHA或仅接受胰岛素治疗相比,SGLT2i治疗与FG住院风险增加在统计学上有显著关联。需要更多研究来证实这些发现。