Department of Epidemiology & Biostatistics, Graduate School of Public Health & Health Policy, City University of New York, New York, New York, United States of America.
OPIK-Research Group for Social Determinants of Health and Demographic Change, University of the Basque Country (UPV/EHU), Bizkaia, Spain.
PLoS One. 2020 Feb 13;15(2):e0228336. doi: 10.1371/journal.pone.0228336. eCollection 2020.
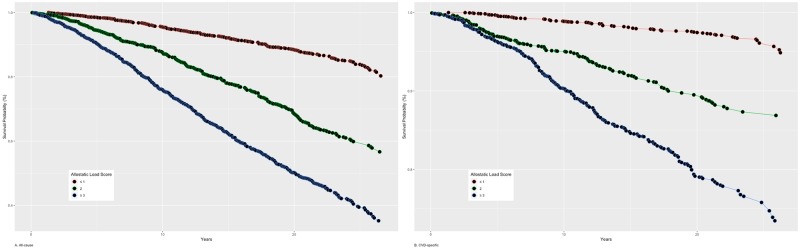
Non-Hispanic blacks have higher mortality rates than non-Hispanic whites whereas Hispanics have similar or lower mortality rates than non-Hispanic blacks and whites despite Hispanics' lower education and access to health insurance coverage. This study examines whether allostatic load, a proxy for cumulative biological risk, is associated with all-cause and cardiovascular (CVD)-specific mortality risks in US adults; and whether these associations vary with race/ethnicity and further with age, sex and education across racial/ethnic groups. Data from the third National Health and Nutritional Examination Survey (NHANES III, 1988-1994) and the 2015 Linked Mortality File were used for adults 25 years or older (n = 13,673 with 6,026 deaths). Cox proportional hazards regression was used to estimate the associations of allostatic load scores (2 and ≥3 relative to ≤1) with a) all-cause and b) CVD-specific mortality risk among NHANES III participants before and after controlling for selected characteristics. Allostatic load scores are associated with higher all-cause and CVD-specific mortality rates among U.S. adults aged 25 years or older, with stronger rates observed for CVD-specific mortality. All-cause mortality rates for each racial/ethnic group differed with age and education whereas for CVD-specific mortality rates, this difference was observed for sex. Our findings of high allostatic load scores associated with all-cause and CVD-specific mortality among US adults call attention to monitor conditions associated with the allostatic load's biomarkers to identify high-risk groups to help monitor social inequities in mortality risk, especially premature mortality.
非西班牙裔黑种人的死亡率高于非西班牙裔白种人,而西班牙裔的死亡率与非西班牙裔黑种人和白种人相似或更低,尽管西班牙裔的受教育程度和获得医疗保险的机会较低。本研究旨在探讨累积生物风险的代理指标——全身适应综合征负荷是否与美国成年人的全因和心血管疾病(CVD)特异性死亡率风险相关;以及这些关联是否因种族/族裔而异,并且在不同种族/族裔群体中是否进一步因年龄、性别和教育程度而异。本研究使用了来自第三次国家健康和营养调查(NHANES III,1988-1994 年)和 2015 年链接死亡率文件的数据,纳入年龄在 25 岁及以上的成年人(n=13673 人,有 6026 人死亡)。使用 Cox 比例风险回归来估计全身适应综合征负荷评分(2 分和≥3 分与≤1 分)与 a)全因和 b)NHANES III 参与者在考虑选定特征之前和之后的 CVD 特异性死亡率风险之间的关联。全身适应综合征负荷评分与美国年龄在 25 岁及以上的成年人的全因和 CVD 特异性死亡率较高相关,CVD 特异性死亡率的相关性更强。每个种族/族裔群体的全因死亡率随年龄和教育程度而不同,而 CVD 特异性死亡率则因性别而不同。本研究发现全身适应综合征负荷评分与美国成年人的全因和 CVD 特异性死亡率较高相关,这提醒人们要关注与全身适应综合征负荷生物标志物相关的疾病,以识别高风险群体,帮助监测死亡率风险中的社会不平等,尤其是过早死亡。