Walsh Thomas L, Taffe Kevin, Sacca Nicole, Bremmer Derek N, Sealey Mary Lynn, Cuevas Elizabeth, Johnston Alexandra, Malarkey Alyson, Behr Rebecca, Embrescia Jessica, Sahota Ekknoor, Loucks Sara, Gupta Nupur, Shields Kelly J, Katz Curren, Kapetanos Anastasios
Department of Medicine, Allegheny General Hospital, Allegheny Health Network, Pittsburgh, PA.
Division of Infectious Diseases, Allegheny General Hospital, Allegheny Health Network, Pittsburgh, PA.
Mayo Clin Proc Innov Qual Outcomes. 2020 Jan 13;4(1):31-39. doi: 10.1016/j.mayocpiqo.2019.09.004. eCollection 2020 Feb.
To determine independent risk factors for inappropriate antibiotic prescribing for acute respiratory tract infections (ARIs) in internal medicine (IM) residency-based primary care offices.
A retrospective study was conducted to measure antibiotic prescribing rates, and multivariable analysis was utilized to identify predictors of inappropriate prescribing among patients presenting to IM residency-based primary care office practices. Patients with an office visit at either of 2 IM residency-based primary care office practices from January 1, 2016, through December 31, 2016, with a primary encounter diagnosis of ARI were included.
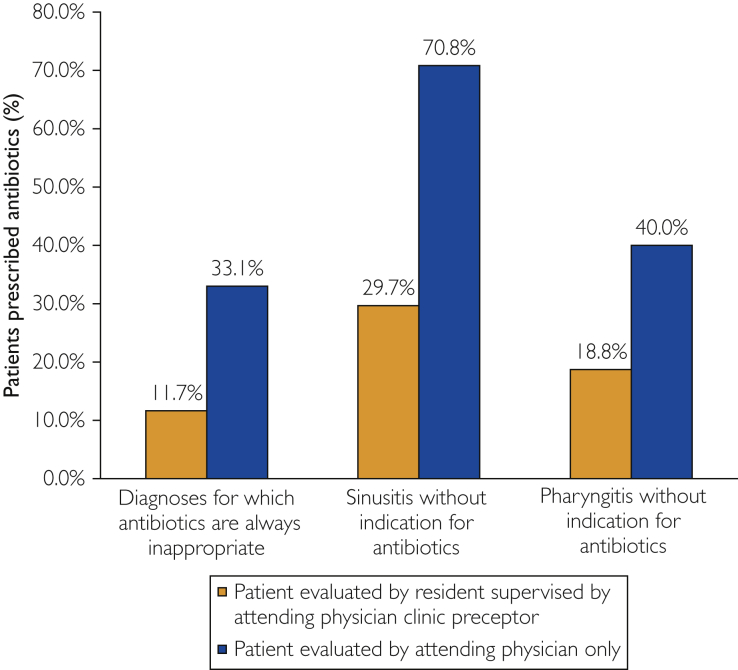
During the study period, 911 unique patient encounters were included with 518 for conditions for which antibiotics were considered always inappropriate. Antibiotics were not indicated in 85.8% (782 of 911) of encounters. However, antibiotics were prescribed in 28.4% (222 of 782) of these encounters. Inappropriate antibiotic prescribing occurred in 111 of 518 (21.4%) encounters for conditions for which antibiotics are always inappropriate. Using multivariable logistic regression analysis to assess for independent risk factors when adjusted for other potential risk factors for office visits at which antibiotics were not indicated, IM resident-associated visits (odds ratio, 0.25; 95% CI, 0.18-0.36) was the only variable independently associated with lower risk of inappropriate antibiotic prescribing.
For ARI visits at which antibiotics were not indicated, IM resident comanagement was associated with lower rates of inappropriate prescribing.
确定在内科住院医师主导的基层医疗诊所中,急性呼吸道感染(ARI)不恰当使用抗生素的独立危险因素。
开展一项回顾性研究以测量抗生素处方率,并采用多变量分析来确定在内科住院医师主导的基层医疗诊所就诊的患者中不恰当处方的预测因素。纳入了2016年1月1日至2016年12月31日期间在两家内科住院医师主导的基层医疗诊所之一就诊、主要就诊诊断为ARI的患者。
在研究期间,共纳入911例独特的患者就诊病例,其中518例所患疾病被认为抗生素使用始终不恰当。在85.8%(911例中的782例)的就诊病例中无需使用抗生素。然而,在这些就诊病例中有28.4%(782例中的222例)开具了抗生素。在518例(21.4%)抗生素使用始终不恰当的就诊病例中发生了不恰当的抗生素处方。在对未开具抗生素的就诊的其他潜在风险因素进行校正后,使用多变量逻辑回归分析评估独立风险因素,与内科住院医师共同管理的就诊(比值比为0.25;95%置信区间为0.18 - 0.36)是与不恰当抗生素处方风险较低独立相关的唯一变量。
对于未开具抗生素的ARI就诊病例,内科住院医师共同管理与较低的不恰当处方率相关。