Pulmonary and Critical Care Medicine Section, VA Boston Healthcare System, Boston, MA, USA; Channing Division of Network Medicine, Brigham & Women's Hospital, Boston, MA, USA; Harvard Medical School, Boston, MA, USA.
Pulmonary and Critical Care Medicine Section, VA Boston Healthcare System, Boston, MA, USA; Harvard Medical School, Boston, MA, USA.
Respir Med. 2020 Feb;162:105878. doi: 10.1016/j.rmed.2020.105878. Epub 2020 Jan 11.
Technology-based physical activity (PA) interventions have been shown to improve daily step counts and health-related quality of life, but their effect on long-term clinical outcomes like acute exacerbations (AEs) is unknown in persons with COPD.
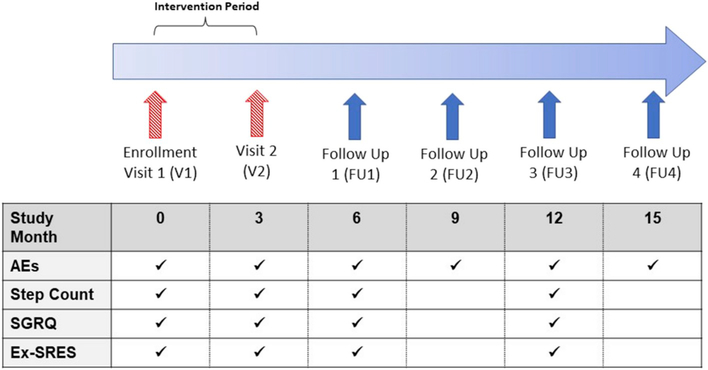
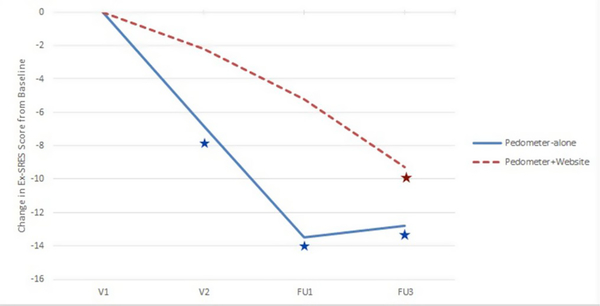
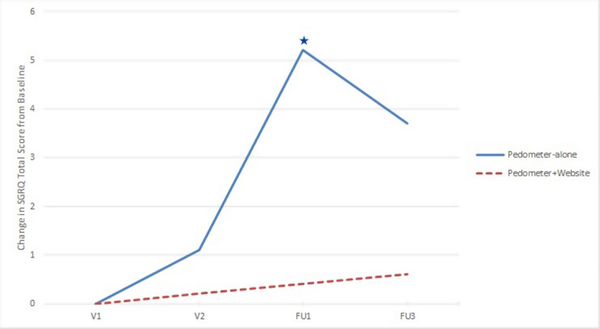
U.S. Veterans with stable COPD were randomized (1:1) to either pedometer alone (control) or pedometer plus a website with feedback, goal-setting, disease education, and a community forum (intervention) for 3 months. AEs were assessed every 3 months over a follow-up period of approximately 15 months. Pedometer-assessed daily step counts, health-related quality-of-life (HRQL), and self-efficacy were assessed at baseline, end-of-intervention at 3 months, and during follow-up approximately 6 and 12 months after enrollment. Zero-inflated Poisson models assessed the effect of the intervention on risk for AEs, compared to controls. Generalized linear mixed-effects models for repeated measures examined between-group and within-group changes in daily step count, HRQL, and self-efficacy.
There were no significant differences in age, FEV% predicted, baseline daily step count, AEs the year prior to enrollment, or duration of follow-up between the intervention (n = 57) and control (n = 52) groups. The intervention group had a significantly reduced risk of AEs (rate ratio = 0.51, [95%CI 0.31-0.85]), compared to the control group. There were no significant between-group differences in change in average daily step count, HRQL, or self-efficacy at 6 and 12 months after enrollment.
A 3-month internet-mediated, pedometer-based PA intervention was associated with reduced risk for AEs of COPD over 12-15 months of follow-up. ClinicalTrials.gov identifier: NCT01772082.
基于技术的身体活动 (PA) 干预已被证明可以提高日常步数和与健康相关的生活质量,但它们对 COPD 患者的急性加重 (AE) 等长期临床结局的影响尚不清楚。
美国稳定期 COPD 退伍军人被随机分为计步器组(对照组)或计步器加网站组(干预组,具有反馈、目标设定、疾病教育和社区论坛功能),干预时长为 3 个月。在大约 15 个月的随访期间,每 3 个月评估一次 AE。在基线、3 个月的干预结束时以及入组后大约 6 个月和 12 个月时,使用计步器评估每日步数、与健康相关的生活质量 (HRQL) 和自我效能。零膨胀泊松模型评估了与对照组相比,干预对 AE 风险的影响。用于重复测量的广义线性混合效应模型检查了每日步数、HRQL 和自我效能的组间和组内变化。
干预组(n=57)和对照组(n=52)在年龄、FEV%预测值、基线每日步数、入组前一年的 AE 发生率或随访时间方面无显著差异。与对照组相比,干预组的 AE 风险显著降低(率比=0.51,[95%CI 0.31-0.85])。入组后 6 个月和 12 个月时,两组间平均每日步数、HRQL 或自我效能的变化均无显著差异。
为期 3 个月的互联网介导、基于计步器的 PA 干预与 12-15 个月随访期间 COPD 急性加重风险降低相关。临床试验注册号:NCT01772082。