Department of Internal Medicine, University of British Columbia, 2775 Laurel St. Vancouver, Vancouver, BC, V5Z 1M9, Canada.
Division of Geriatric Medicine, University of Ottawa, Ottawa, Canada.
BMC Geriatr. 2020 Feb 14;20(1):62. doi: 10.1186/s12877-020-1462-y.
"Failure to thrive" and associated diagnoses are non-specific terms applied to older adults when there is lack of diagnostic clarity and imply an absence of medical acuity. We investigated the effect of such admission diagnoses on delivery of patient care in a cohort of older adults admitted to a tertiary care teaching hospital.
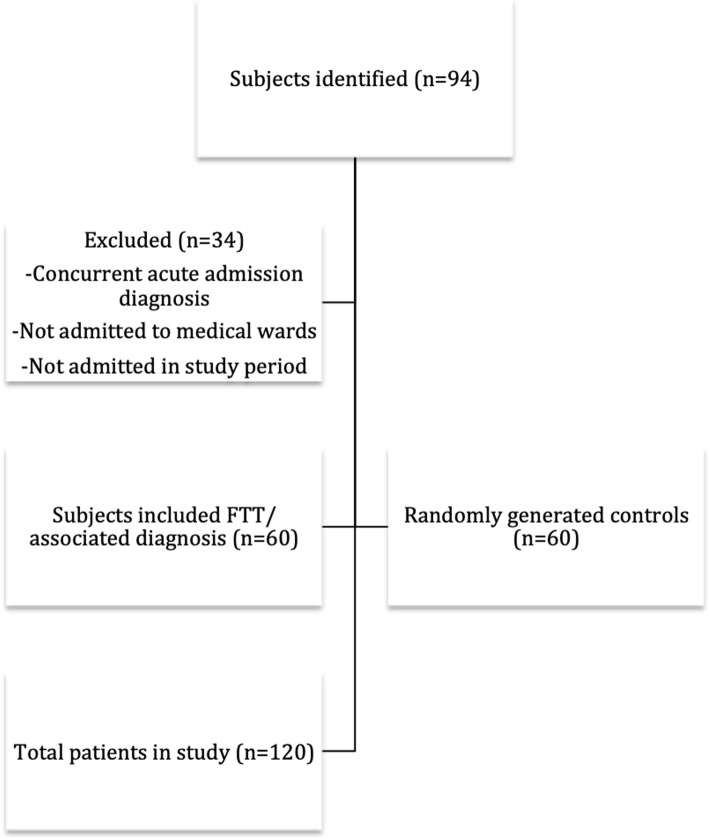
Retrospective matched cohort study conducted at a tertiary care hospital in Vancouver, BC. Cases identified were adults aged ≥65 years admitted to acute medical wards with an admission diagnosis of "failure to thrive", "FTT", "failure to cope", or "FTC", between January 1, 2016 and November 1, 2017 (n = 60, median age 80 years). Age-matched controls met the same inclusion criteria with admission diagnoses other than those of interest (n = 60, median age 79 years).
The primary outcome was time to admission, measured from time points in the emergency room that spanned from triage to completion of admission orders. Secondary outcomes were concordance of admission and discharge diagnoses and length of stay in hospital. The total time from triage to admission for older adults admitted with FTT and associated diagnoses was 10 h 40 min, compared to 6 h 58 min for controls (p = .02). Concordance of admission and discharge diagnoses was only 12% for the "failure to thrive" cohort, and 95% for controls. Notably, 88% of the "failure to thrive" cohort had an acute medical diagnosis at the time of discharge. Patients in this cohort stayed 18.3 days in hospital compared to 10.2 days (p = .001).
Patients with an admission diagnosis of FTT or other associated diagnoses had significant delays in care when presenting to the emergency room, despite often having acute medical conditions on presentation. The use of this non-specific label can lead to premature diagnostic closure and should be avoided in clinical practice.
“生长迟缓”和相关诊断是用于老年人的非特异性术语,当缺乏明确的诊断时使用,并且暗示缺乏医疗敏锐度。我们调查了这种入院诊断对在温哥华的一家三级护理教学医院收治的老年患者护理的影响。
在不列颠哥伦比亚省温哥华的一家三级护理医院进行回顾性匹配队列研究。病例是在 2016 年 1 月 1 日至 2017 年 11 月 1 日期间因“生长迟缓”、“FTT”、“无法应对”或“FTC”等入院诊断而被收治到急性内科病房的年龄≥65 岁的成年人(n=60,中位年龄 80 岁)。年龄匹配的对照组符合相同的纳入标准,但入院诊断不是我们感兴趣的诊断(n=60,中位年龄 79 岁)。
主要结果是入院时间,从急诊科的分诊时间到完成入院医嘱的时间进行测量。次要结果是入院和出院诊断的一致性以及住院时间。与对照组相比,因 FTT 和相关诊断而入院的老年人从分诊到入院的总时间为 10 小时 40 分钟,而对照组为 6 小时 58 分钟(p=0.02)。“生长迟缓”组入院和出院诊断的一致性仅为 12%,而对照组为 95%。值得注意的是,“生长迟缓”组中有 88%的患者在出院时患有急性内科疾病。该队列的患者在医院住院 18.3 天,而对照组为 10.2 天(p=0.001)。
尽管在就诊时常常存在急性内科疾病,但因“生长迟缓”或其他相关诊断而入院的患者在就诊到急诊科时的护理时间明显延迟。使用这种非特异性标签可能会导致过早的诊断结束,在临床实践中应避免使用。