Oxford University Clinical Research Unit, Wellcome Trust Asia Programme, Ho Chi Minh City, Vietnam.
University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam.
BMC Med. 2020 Feb 17;18(1):35. doi: 10.1186/s12916-020-1496-1.
Dengue infection can cause a wide spectrum of clinical outcomes. The severe clinical manifestations occur sufficiently late in the disease course, during day 4-6 of illness, to allow a window of opportunity for risk stratification. Markers of inflammation may be useful biomarkers. We investigated the value of C-reactive protein (CRP) measured early on illness days 1-3 to predict dengue disease outcome and the difference in CRP levels between dengue and other febrile illnesses (OFI).
We performed a nested case-control study using the clinical data and samples collected from the IDAMS-consortium multi-country study. This was a prospective multi-center observational study that enrolled almost 8000 participants presenting with a dengue-like illness to outpatient facilities in 8 countries across Asia and Latin America. Predefined severity definitions of severe and intermediate dengue were used as the primary outcomes. A total of 281 cases with severe/intermediate dengue were compared to 836 uncomplicated dengue patients as controls (ratio 1:3), and also 394 patients with OFI.
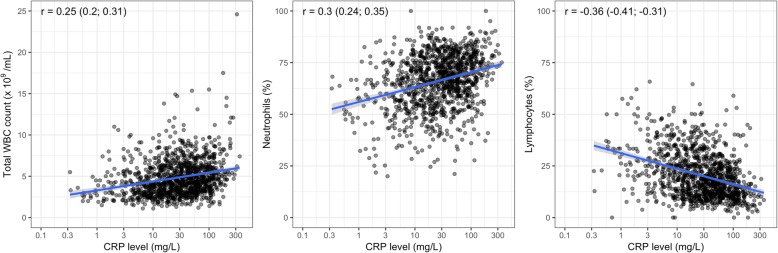
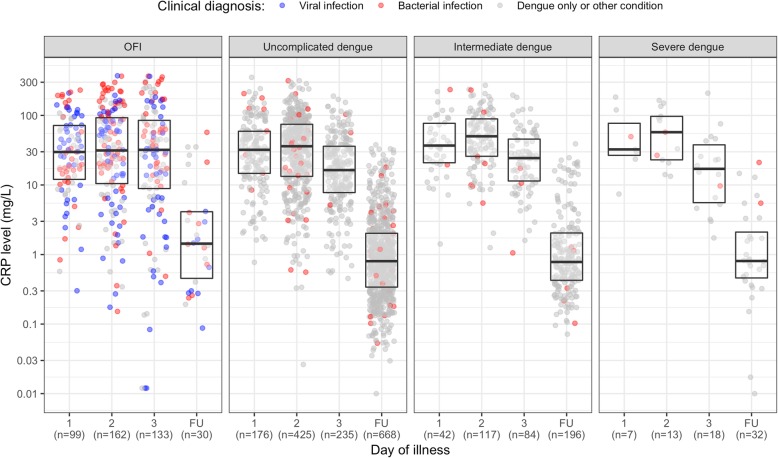
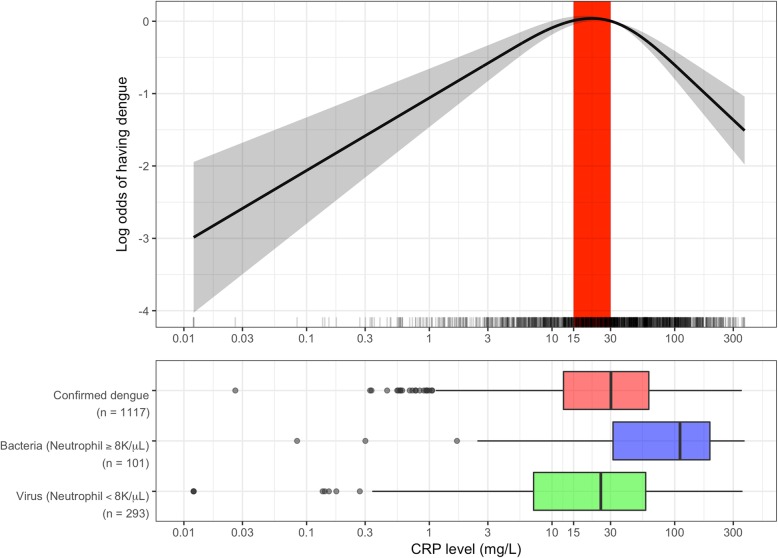
In patients with confirmed dengue, median (interquartile range) of CRP level within the first 3 days was 30.2 mg/L (12.4-61.2 mg/L) (uncomplicated dengue, 28.6 (10.5-58.9); severe or intermediate dengue, 34.0 (17.4-71.8)). Higher CRP levels in the first 3 days of illness were associated with a higher risk of severe or intermediate outcome (OR 1.17, 95% CI 1.07-1.29), especially in children. Higher CRP levels, exceeding 30 mg/L, also associated with hospitalization (OR 1.37, 95% CI 1.14-1.64) and longer fever clearance time (HR 0.84, 95% CI 0.76-0.93), especially in adults. CRP levels in patients with dengue were higher than patients with potential viral infection but lower than patients with potential bacterial infection, resulting in a quadratic association between dengue diagnosis and CRP, with levels of approximately 30 mg/L associated with the highest risk of having dengue. CRP had a positive correlation with total white cell count and neutrophils and negative correlation with lymphocytes, but did not correlate with liver transaminases, albumin, or platelet nadir.
In summary, CRP measured in the first 3 days of illness could be a useful biomarker for early dengue risk prediction and may assist differentiating dengue from other febrile illnesses.
登革热感染可导致广泛的临床结局。严重的临床表现发生在疾病的第 4-6 天,足以在风险分层方面提供机会窗口。炎症标志物可能是有用的生物标志物。我们研究了在疾病第 1-3 天早期测量 C 反应蛋白(CRP)来预测登革热疾病结局的价值,以及 CRP 水平在登革热与其他发热性疾病(OFI)之间的差异。
我们使用 IDAMS 联盟多中心研究中收集的临床数据和样本进行了嵌套病例对照研究。这是一项前瞻性多中心观察性研究,在亚洲和拉丁美洲 8 个国家的门诊设施招募了近 8000 名出现登革热样疾病的患者。严重和中度登革热的预先定义严重程度定义被用作主要结局。将 281 例严重/中度登革热病例与 836 例无并发症登革热患者作为对照(比例 1:3)进行比较,还与 394 例 OFI 患者进行了比较。
在确诊登革热的患者中,第 1-3 天内 CRP 水平的中位数(四分位距)为 30.2mg/L(12.4-61.2mg/L)(无并发症登革热患者为 28.6mg/L(10.5-58.9);严重或中度登革热患者为 34.0mg/L(17.4-71.8))。在疾病的第 1-3 天内,CRP 水平升高与严重或中度结局的风险增加相关(OR 1.17,95%CI 1.07-1.29),尤其是在儿童中。在第 1-3 天内 CRP 水平升高,超过 30mg/L,也与住院(OR 1.37,95%CI 1.14-1.64)和发热清除时间延长(HR 0.84,95%CI 0.76-0.93)相关,尤其是在成人中。登革热患者的 CRP 水平高于潜在病毒感染患者,但低于潜在细菌感染患者,导致登革热诊断与 CRP 之间呈二次关联,CRP 水平约为 30mg/L 时与登革热风险最高相关。CRP 与总白细胞计数和中性粒细胞呈正相关,与淋巴细胞呈负相关,但与肝转氨酶、白蛋白或血小板最低点无关。
综上所述,在疾病的第 1-3 天内测量的 CRP 可能是早期登革热风险预测的有用生物标志物,有助于区分登革热与其他发热性疾病。