Yip Benjamin Cherng Hann, Sayeed Sajjad Hossain, Wang Jie-Xun, Anastassiades Constantinos P
Department of General Medicine, Khoo Teck Puat Hospital, Singapore 768828, Singapore.
Department of Acute Medicine, Northampton General Hospital, Cliftonville, Northampton NN1 5BD, United Kingdom.
World J Gastrointest Endosc. 2020 Feb 16;12(2):72-82. doi: 10.4253/wjge.v12.i2.72.
In nonvariceal upper gastrointestinal bleeding (NVUGIB), the optimal volume of adrenaline, the optimal number of hemoclips, and the application of thermal coagulation in determining patient outcomes have not been well studied.
To demonstrate a dose-response relationship between the commonly used endoscopic modalities for the treatment of non-variceal upper gastrointestinal bleeding and various clinical outcomes.
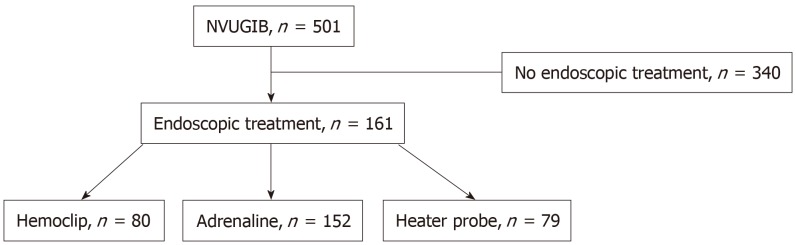
Patients presenting with NVUGIB were retrospectively identified and analyzed. These patients were stratified as follows: (1) > 10 mL of adrenaline injected ≤ 10 mL; (2) > 1 hemoclip placed ≤ 1 hemoclip; (3) Heater probe used or not; and (4) > 2 treatment modalities used ≤ 2. The primary outcomes were rebleeding and the need for repeat endoscopy. The secondary outcomes were the need for surgery, required transfusions, length of hospital stay, death during the same admission period and 30 d mortality. Patients with NVUGIB who required endoscopic therapy were included. Those who did not require endoscopic therapy or were initially treated with surgery or embolization were excluded.
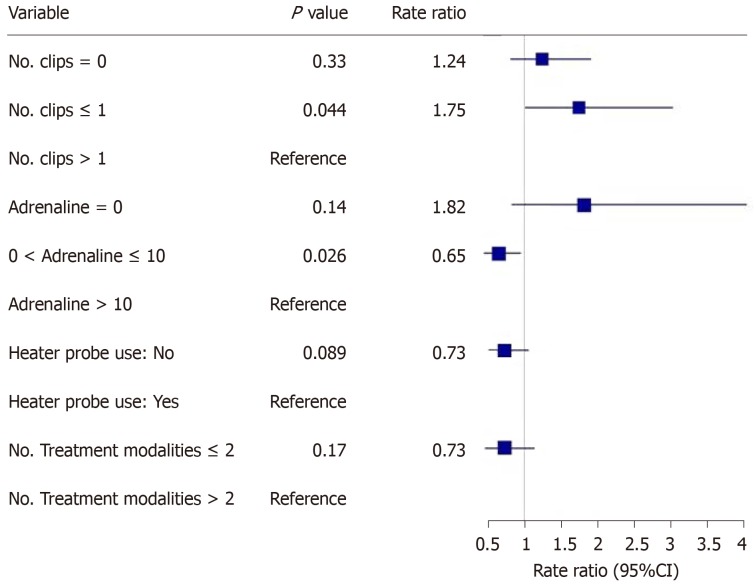
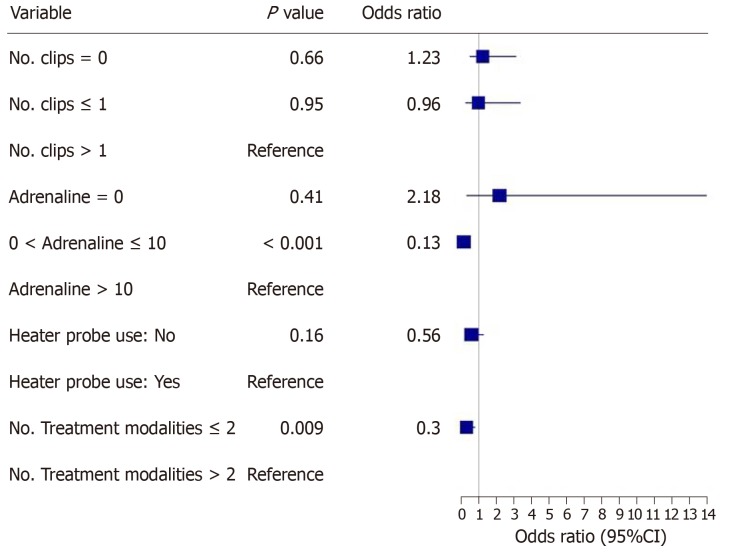
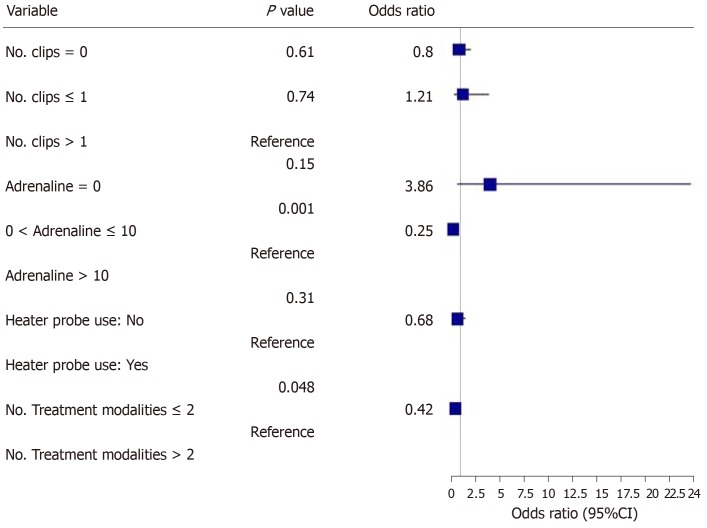
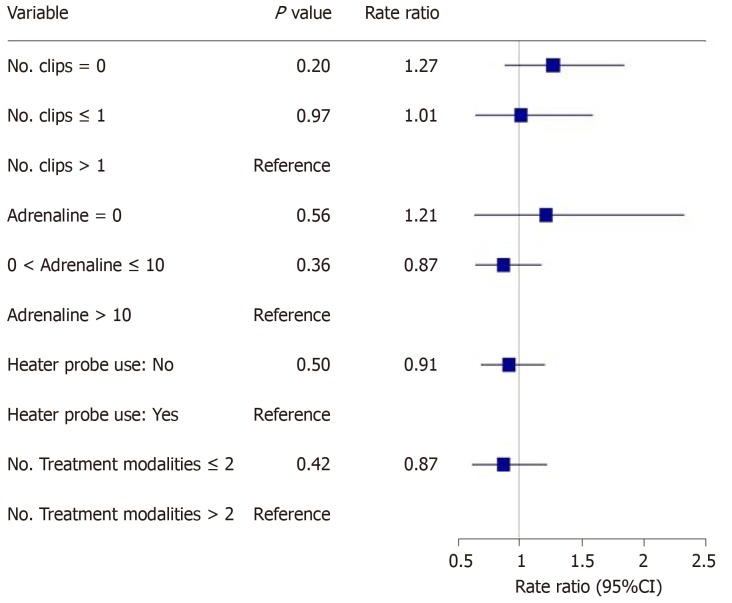
In all, 501 patients with NVUGIB were treated. One hundred sixty-one (32.1%) patients needed endoscopic therapy. The injection of < 10 mL of adrenaline was associated with less rebleeding ( < 0.0001), the need for repeat endoscopy ( = 0.001) and a decreased length of hospital stay ( = 0.026). The use of > 2 treatment modalities were associated with increased rebleeding ( = 0.009) and the need for repeat endoscopy ( = 0.048). The placement of > 1 hemoclip was associated with a decreased length of hospital stay ( = 0.044). The rates of surgery and death were low, and there were no other significant differences between the patient groups.
The more restrictive use of adrenaline and number of endoscopic modalities to treat NVUGIB with the more liberal use of hemoclips was associated with better patient outcomes.
在非静脉曲张性上消化道出血(NVUGIB)中,肾上腺素的最佳用量、止血夹的最佳数量以及热凝治疗在确定患者预后方面尚未得到充分研究。
证明治疗非静脉曲张性上消化道出血常用的内镜治疗方式与各种临床结局之间的剂量反应关系。
对出现NVUGIB的患者进行回顾性识别和分析。这些患者按以下方式分层:(1)注射肾上腺素>10 mL与≤10 mL;(2)放置止血夹>1个与≤1个;(3)使用或未使用热活检钳;(4)使用>2种治疗方式与≤2种。主要结局为再出血和重复内镜检查的必要性。次要结局为手术需求、所需输血、住院时间、同一住院期间死亡及30天死亡率。纳入需要内镜治疗的NVUGIB患者。排除那些不需要内镜治疗或最初接受手术或栓塞治疗的患者。
总共治疗了501例NVUGIB患者。161例(32.1%)患者需要内镜治疗。注射<10 mL肾上腺素与较少的再出血(<0.0001)、重复内镜检查的必要性(=0.001)及住院时间缩短(=0.026)相关。使用>2种治疗方式与再出血增加(=0.009)和重复内镜检查的必要性(=0.048)相关。放置>1个止血夹与住院时间缩短(=0.044)相关。手术率和死亡率较低,患者组之间无其他显著差异。
更严格地使用肾上腺素和内镜治疗方式数量,同时更广泛地使用止血夹治疗NVUGIB与更好的患者预后相关。