Department of Anaesthesia, Austin Health, Heidelberg, Victoria, Australia.
The Department of Medicine, Austin Health, The Univesity of Melbourne, Heidelberg, Victoria, Australia.
BMJ Open. 2020 Feb 16;10(2):e029159. doi: 10.1136/bmjopen-2019-029159.
The effects of hypercapnia on regional cerebral oxygen saturation (rSO) during surgery are unclear. We conducted a randomised controlled trial to investigate the relationship between mild hypercapnia and rSO. We hypothesised that, compared with targeted normocapnia (TN), targeted mild hypercapnia (TMH) during major surgery would increase rSO.
A prospective, randomised, controlled trial in adult participants undergoing elective major surgery.
A single tertiary centre in Heidelberg, Victoria, Australia.
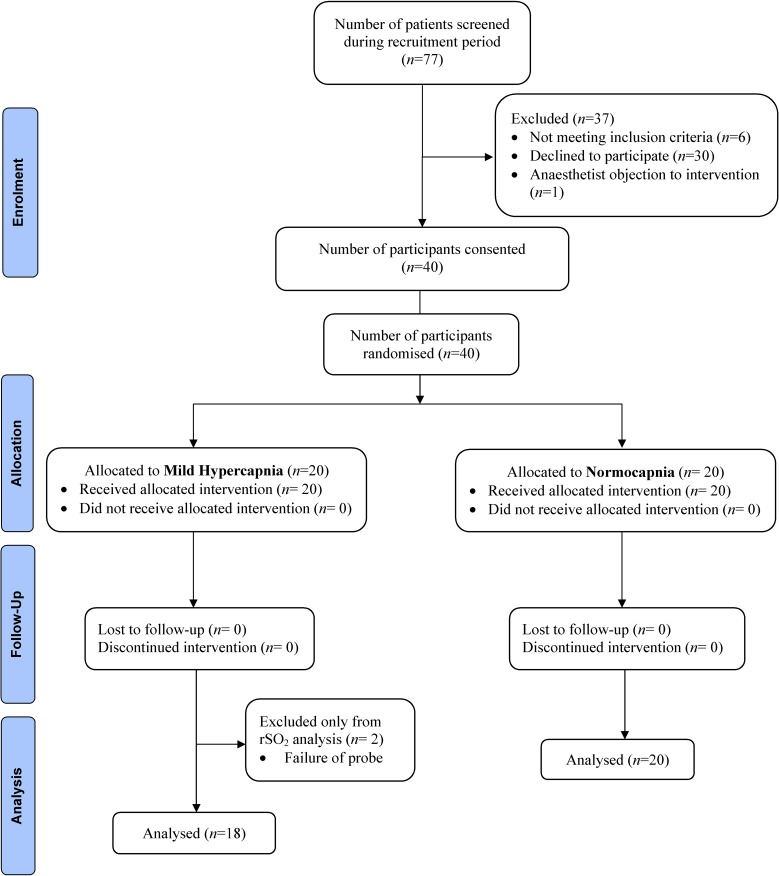
40 participants were randomised to either a TMH or TN group (20 to each).
TMH (partial pressure of carbon dioxide in arterial blood, PaCO, 45-55 mm Hg) or TN (PaCO 35-40 mm Hg) was delivered via controlled ventilation throughout surgery.
The primary endpoint was the absolute difference between the two groups in percentage change in rSO from baseline to completion of surgery. Secondary endpoints included intraoperative pH, bicarbonate concentration, base excess, serum potassium concentration, incidence of postoperative delirium and length of stay (LOS) in hospital.
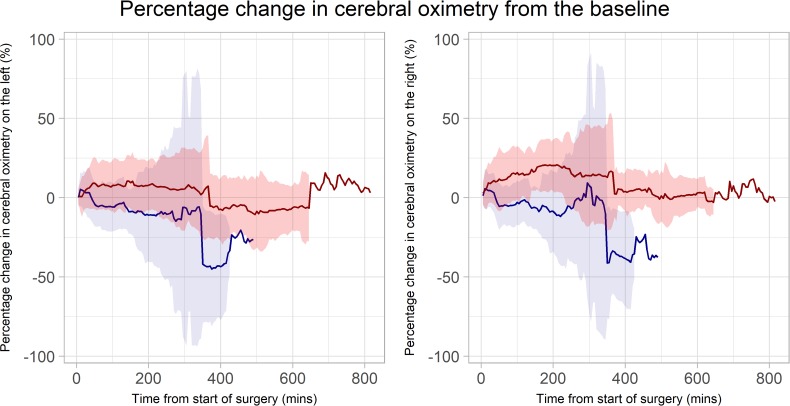
The absolute difference between the two groups in percentage change in rSO from the baseline to the completion of surgery was 19.0% higher in both hemispheres with TMH (p<0.001). On both sides, the percentage change in rSO was greater in the TMH group than the TN group throughout the duration of surgery. The difference between the groups became more noticeable over time. Furthermore, postoperative delirium was higher in the TN group (risk difference 0.3, 95% CI 0.1 to 0.5, p=0.02). LOS was similar between groups (5 days vs 5 days; p=0.99).
TMH was associated with a stable increase in rSO from the baseline, while TN was associated with a decrease in rSO in both hemispheres in patients undergoing major surgery. This resulted in a clear separation of percentage change in rSO from the baseline between TMH and TN over time. Our findings provide the rationale for larger studies on TMH during surgery.
The Australian New Zealand Clinical Trials Registry (ACTRN12616000320459).
围手术期高碳酸血症对局部脑氧饱和度(rSO)的影响尚不清楚。我们进行了一项随机对照试验,以研究轻度高碳酸血症与 rSO 之间的关系。我们假设,与目标正常碳酸血症(TN)相比,在大型手术中进行目标轻度高碳酸血症(TMH)将增加 rSO。
一项在澳大利亚维多利亚州海德堡的一家单一三级中心进行的前瞻性、随机、对照试验。
40 名参与者被随机分配到 TMH 或 TN 组(每组 20 名)。
通过控制通气在整个手术过程中向 TMH(动脉血二氧化碳分压,PaCO 2 45-55mmHg)或 TN(PaCO 2 35-40mmHg)输送。
主要终点是从基线到手术完成时两组之间 rSO 变化的绝对差异。次要终点包括术中 pH 值、碳酸氢盐浓度、碱剩余、血清钾浓度、术后谵妄发生率和住院时间( LOS )。
TMH 时双侧半球 rSO 从基线到手术完成的变化百分比绝对差值高 19.0%(p<0.001)。在整个手术过程中,TMH 组 rSO 的变化百分比大于 TN 组。随着时间的推移,两组之间的差异变得更加明显。此外,TN 组术后谵妄发生率较高(风险差异 0.3,95%CI 0.1 至 0.5,p=0.02)。两组 LOS 相似(5 天与 5 天;p=0.99)。
TMH 与 rSO 从基线开始的稳定增加相关,而 TN 与双侧半球 rSO 的降低相关,这导致 rSO 从基线开始的变化百分比在 TMH 和 TN 之间随着时间的推移明显分离。我们的研究结果为围手术期 TMH 的更大规模研究提供了依据。
澳大利亚和新西兰临床试验注册中心(ACTRN12616000320459)。