Department of Thoracic Surgery, Shanghai Chest Hospital, Shanghai Jiao Tong University, Huaihaixi Road 241, Shanghai, 200030, People's Republic of China.
Department of Thoracic Surgery, Xinxiang Central Hospital, Xinxiang, 453000, Henan Province, People's Republic of China.
Surg Endosc. 2021 Feb;35(2):593-601. doi: 10.1007/s00464-020-07420-y. Epub 2020 Feb 18.
We analyzed the pathological characteristics and recurrence pattern of cN0 submucosal esophageal cancer after esophagectomy and conducted risk stratification to determine the feasibility of performing endoscopic resection for cN0pT1b esophageal squamous cell malignancies.
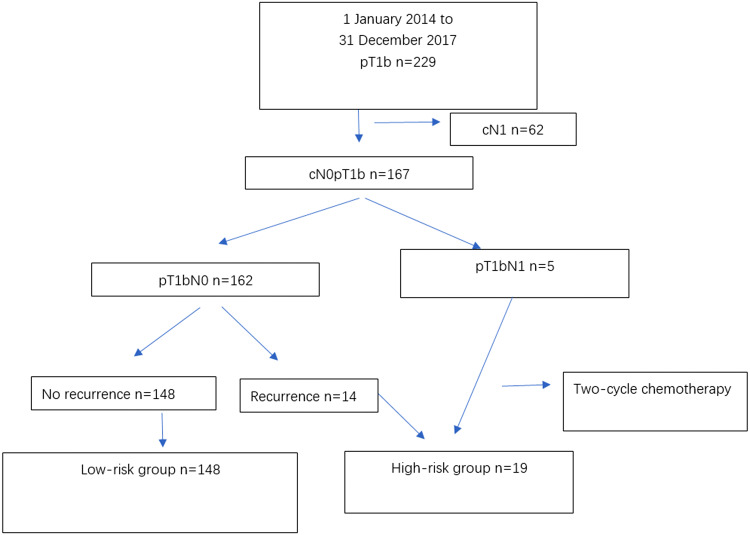
We retrospectively enrolled 167 patients who underwent right-sided transthoracic esophagectomy and extended thoracic/abdominal two-field lymphadenectomy. Patients with pathologically confirmed lymph node metastasis or tumor recurrence constituted the high-risk group for endoscopic submucosal resection, and the remainder were defined as low risk. Factors affecting lymphatic metastasis and long-term recurrence were identified by univariate and multivariate analyses.
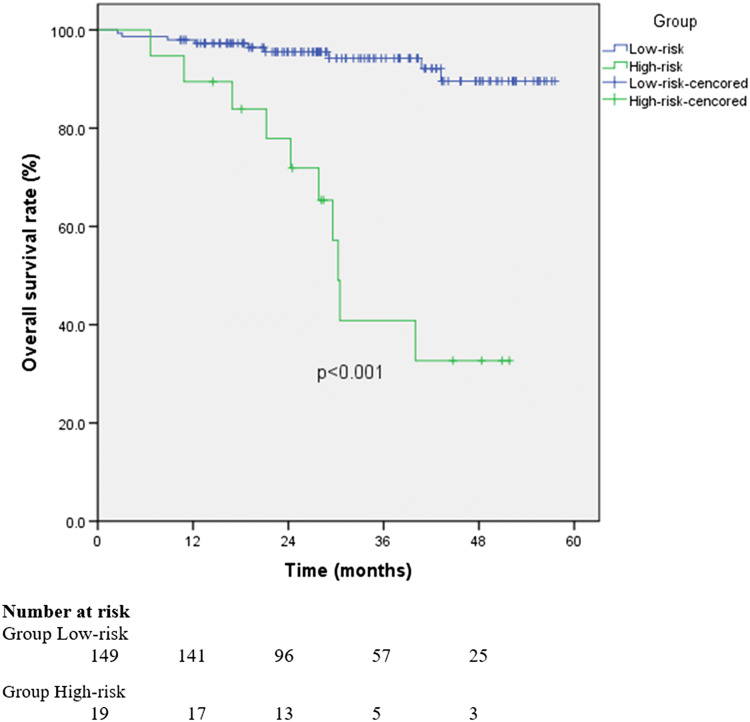
Postoperative pathology showed that five patients (5/167; 3%) had lymph node metastases. Follow-up ranged from 12-60 months, with a median of 29 months. A total of 17 patients (10.2%) had recurrences during follow-up, including three patients with pathologic nodal metastasis (pN +) found at surgery. Invasion depth, differentiation, and tumor size differed significantly in high-risk patients. Overall 3-year survival rates were 94.2% (low-risk) and 40.9% (high-risk) (p < 0.01). Twenty-one patients with sm1 cancer, high tumor differentiation, and tumor length < 2 cm had no lymph node metastasis or lymphovascular invasion, and none of these patients experienced recurrence.
Endoscopic submucosal resection alone may be feasible for patients with small (≤ 2 cm) clinically N0 submucosal esophageal squamous cell carcinoma with low invasion depth (sm1) and higher differentiation, but prospective studies are required for confirmation. Other patients require surgical resection with extended two-field thoracic/abdominal lymphadenectomy.
我们分析了食管切除术后 cN0 黏膜下食管癌的病理特征和复发模式,并进行了风险分层,以确定 cN0pT1b 食管鳞癌行内镜下切除的可行性。
我们回顾性纳入了 167 例接受右胸经胸食管切除术和扩大的胸/腹两野淋巴结清扫术的患者。病理证实有淋巴结转移或肿瘤复发的患者构成内镜黏膜下切除的高危组,其余患者定义为低危组。通过单因素和多因素分析确定影响淋巴转移和长期复发的因素。
术后病理显示 5 例(5/167;3%)患者有淋巴结转移。随访时间为 12-60 个月,中位随访时间为 29 个月。随访期间共有 17 例(10.2%)患者复发,其中 3 例在手术时发现病理淋巴结转移(pN+)。高危组患者的浸润深度、分化程度和肿瘤大小差异有统计学意义。总体 3 年生存率分别为 94.2%(低危组)和 40.9%(高危组)(p<0.01)。21 例 sm1 期、高分化、肿瘤长度<2cm 的 sm1 期癌症患者无淋巴结转移或血管淋巴管侵犯,均未复发。
对于小(≤2cm)、临床 N0 黏膜下、低浸润深度(sm1)和高分化的食管鳞癌患者,单独行内镜黏膜下切除术可能是可行的,但需要前瞻性研究来证实。其他患者需要行扩大的胸/腹两野淋巴结清扫术的手术切除。