Department of Oncologic and General Surgery, University Hospital in Olsztyn, Olsztyn, Poland.
Department of Laboratory Medicine, University Hospital in Olsztyn, Olsztyn, Poland.
BMC Cancer. 2020 Feb 19;20(1):133. doi: 10.1186/s12885-020-6590-4.
The importance of ACF is not fully explained, however, their number may be a good predictor of synchronous and metachronic adenoma or other polyps whose removal reduces the risk of CRC. Due to the epidemiological and genetic association of ACF with pre-cancer lesions, they may be a potential CRC biomarker. The aim of our study was to show that the number and type of rectal ACF may be a good predictive factor for the presence of polyps located proximally from the splenic flexure and that the type and number of ACF can correlate with the number and specific types of polyps in the large intestine.
The study included 131 patients who underwent colonoscopy combined with rectal mucosa staining with 0.25% methylene blue. The number of rectal ACF was determined and bioptats were sampled for histopathological examination to assess the type of ACF. Endoscopic ACF assessment criteria given by L. Roncucci were used. The obtained material was subjected to statistical analysis using probability distribution, U-test, t-student test, and chi as well as the Statistica 7.1 software package.
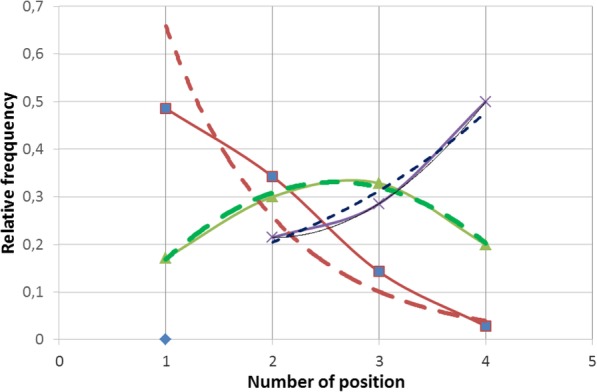
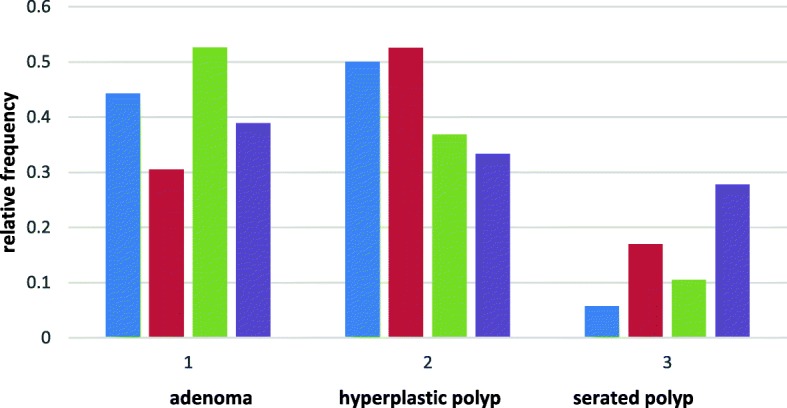
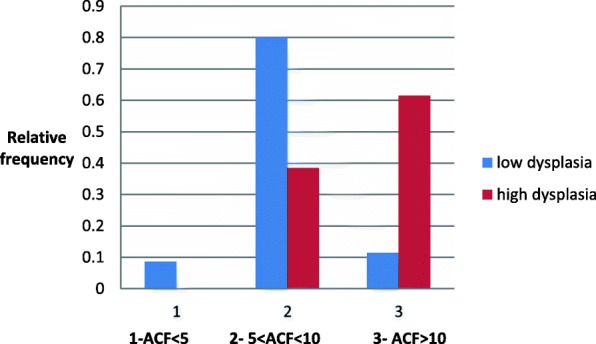
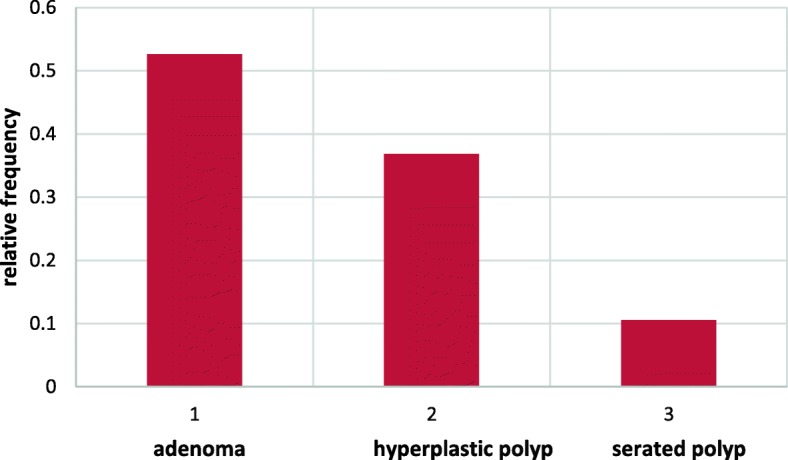
The study population was divided into three subgroups according to the number of ACF observed, i.e. ACF < 5, 5-10 and > 10. ACF < 5 were found in 35 patients (29.41%), 5-10 ACF in 70 (58.82%) and ACF > 10 in 14 individuals (11.76%). The study revealed the presence of normal ACF (p = 0.49), hyperplastic ACF (p = 0.34), dysplastic ACF (p = 0.11), and mixed ACF (p = 0.06). A single type of ACF was most commonly observed (n = 88, p = 0.74). In the researched group a larger number of ACF is concurrent with adenomas and hyperplastic polyps. The number of ACF clearly correlates with the dysplasia advancement in the adenoma and the number of polyps found.
Rectal ACF are a useful marker for the presence of cancerous lesions in the proximal and distal sections of the large intestine.
ACF 的重要性尚未得到充分解释,但其数量可能是预测同步和异时性腺瘤或其他息肉的良好指标,这些息肉的切除可降低 CRC 的风险。由于 ACF 与癌前病变在流行病学和遗传学上的关联,它们可能是 CRC 的潜在生物标志物。我们的研究旨在表明直肠 ACF 的数量和类型可能是预测脾曲近端存在息肉的良好预测因子,并且 ACF 的类型和数量可以与大肠中息肉的数量和特定类型相关。
该研究纳入了 131 名接受结肠镜检查并结合直肠黏膜 0.25%亚甲蓝染色的患者。确定直肠 ACF 的数量并进行活检以进行组织病理学检查以评估 ACF 的类型。使用 L. Roncucci 给出的内镜 ACF 评估标准。使用概率分布、U 检验、t 检验和卡方以及 Statistica 7.1 软件包对获得的材料进行统计分析。
根据观察到的 ACF 数量,将研究人群分为三个亚组,即 ACF<5、5-10 和>10。在 35 名患者(29.41%)中发现 ACF<5,在 70 名患者(58.82%)中发现 5-10 个 ACF,在 14 名患者(11.76%)中发现>10 个 ACF。研究表明存在正常的 ACF(p=0.49)、增生性 ACF(p=0.34)、发育不良性 ACF(p=0.11)和混合性 ACF(p=0.06)。最常见的是观察到单一类型的 ACF(n=88,p=0.74)。在研究组中,ACF 数量越多,腺瘤和增生性息肉的数量就越多。ACF 的数量与腺瘤中的发育不良进展以及发现的息肉数量明显相关。
直肠 ACF 是大肠近端和远端癌性病变的有用标志物。