Putora Paul Martin, Leskow Pawel, McDonald Fiona, Batchelor Tim, Evison Matthiew
Dept of Radiation Oncology, Kantonsspital St Gallen, St Gallen, Switzerland.
Dept of Radiation Oncology, University of Bern, Bern, Switzerland.
ERJ Open Res. 2020 Feb 17;6(1). doi: 10.1183/23120541.00159-2019. eCollection 2020 Jan.
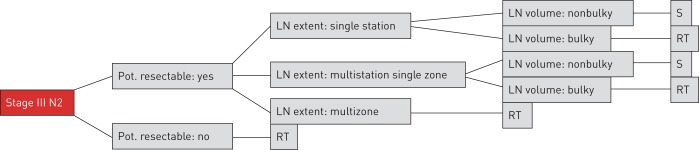
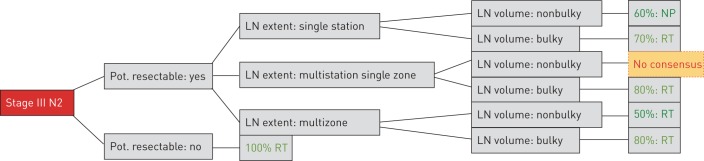
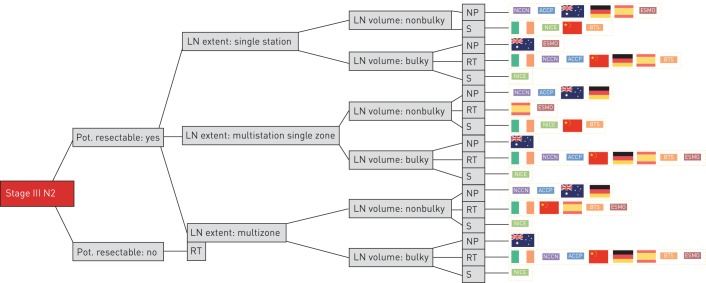
Stage III N2 nonsmall cell lung cancer (NSCLC) is a complex disease with poor treatment outcomes. For patients in whom the disease is considered technically resectable, the main treatment options include surgery (with neoadjuvant or adjuvant chemotherapy/neoadjuvant chemoradiotherapy (CRT)) or CRT followed by adjuvant immunotherapy (dependent on programmed death ligand 1 status). As there is no clear evidence demonstrating a survival benefit between these options, patient preference plays an important role. A lack of a consensus definition of resectability of N2 disease adds to the complexity of the decision-making process. We compared 10 international guidelines on the treatment of NSCLC to investigate the recommendations on preoperatively diagnosed stage III N2 NSCLC. This comparison simplified the treatment paths to multimodal therapy based on surgery or radiotherapy (RT). We analysed factors relevant to decision-making within these guidelines. Overall, for nonbulky mediastinal lymph node involvement there was no clear preference between surgery and CRT. With increasing extent of mediastinal nodal disease, a tendency towards multimodal treatment based on RT was identified. In multiple scenarios, surgery or RT-based treatments are feasible and patient involvement in decision-making is critical.
Ⅲ期N2非小细胞肺癌(NSCLC)是一种治疗效果不佳的复杂疾病。对于那些被认为在技术上可切除的患者,主要治疗选择包括手术(联合新辅助或辅助化疗/新辅助放化疗(CRT))或CRT后序贯辅助免疫治疗(取决于程序性死亡配体1状态)。由于没有明确证据表明这些选择之间存在生存获益差异,患者偏好起着重要作用。N2疾病可切除性缺乏共识定义增加了决策过程的复杂性。我们比较了10项关于NSCLC治疗的国际指南,以研究术前诊断为Ⅲ期N2 NSCLC的治疗建议。这种比较简化了基于手术或放疗(RT)的多模式治疗路径。我们分析了这些指南中与决策相关的因素。总体而言,对于非巨大纵隔淋巴结受累,手术和CRT之间没有明确偏好。随着纵隔淋巴结疾病范围的增加,发现了基于RT的多模式治疗趋势。在多种情况下,基于手术或RT的治疗是可行的,患者参与决策至关重要。