Hôpital Saint-Louis, Assistance Publique Hôpitaux de Paris, Paris, France.
INSERM, Villejuif, France.
J Int AIDS Soc. 2020 Feb;23(2):e25420. doi: 10.1002/jia2.25420.
Daily pre-exposure prophylaxis (PrEP) with tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) is associated with a small but statistically significant decrease in estimated glomerular filtration rate (eGFR). We assessed the renal safety of on-demand PrEP with TDF/FTC in HIV-1 uninfected men.
We used data from the randomized double-blind placebo-controlled ANRS-IPERGAY trial and its open-label extension conducted between February 2012 and June 2016 among HIV-uninfected MSM starting on-demand PrEP. Using linear mixed model, we evaluated the mean eGFR decline from baseline over time and determined risks factors associated with eGFR decline during the study.
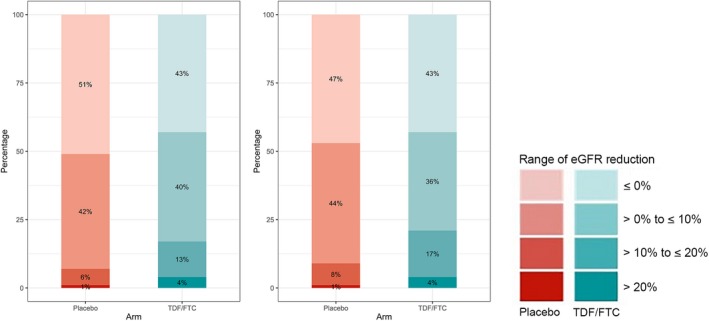
During the blind phase, with a median follow-up of 9.4 months, the mean decline slope of eGFR from baseline was -0.88 and -1.53 mL/min/1.73 m per year in the placebo (n = 201) and the TDF/FTC group (n = 198) respectively, with a slope difference of 0.65 mL/min/1.73 m per year (p = 0.27). Including both phases, 389 participants started on-demand TDF/FTC with a median follow-up of 19.2 months and a mean decline of eGFR from baseline of -1.14 mL/min/1.73 m per year (p < 0.001). The slope of eGFR reduction was not significantly different in participants with baseline eGFR ≤ 90 mL/min/1.73 m (p = 0.44), age >40 years (p = 0.24) or hypertension (p = 0.21). There was a dose-response relationship between recent tenofovir exposure and lower eGFR when considering the number of pills taken in the two months prior the visit (eGFR difference of -0.88 mL/min/1.73 m between >15 pills/month vs. ≤15 pills/month, p < 0.01) or plasma tenofovir concentrations at the visit (eGFR difference compared to ≤2 ng/mL: >2 to ≤10ng/mL: -0.98 mL/min/1.73 m , >10 to ≤40ng/mL: -1.28 mL/min/1.73 m , >40 ng/mL: -1.82 mL/min/1.73 m , p < 0.001). Three participants discontinued TDF/FTC for eGFR < 60 mL/min/1.73 m during the OLE phase. No case of Fanconi syndrome was reported.
The renal safety of on-demand PrEP with TDF/FTC was good. The overall reduction and intermittent exposure to TDF/FTC may explain this good renal safety.
每日使用替诺福韦二吡呋酯/恩曲他滨(TDF/FTC)进行暴露前预防(PrEP)与肾小球滤过率(eGFR)的估计值略有但具有统计学意义的下降有关。我们评估了 HIV-1 未感染者使用 TDF/FTC 按需 PrEP 的肾脏安全性。
我们使用了 2012 年 2 月至 2016 年 6 月间进行的随机双盲安慰剂对照 ANRS-IPERGAY 试验及其开放标签扩展的数据,该试验纳入了开始按需 PrEP 的 HIV-未感染者中的男男性行为者。我们使用线性混合模型评估了从基线到随访期间 eGFR 的平均下降斜率,并确定了研究期间与 eGFR 下降相关的危险因素。
在盲法阶段,中位随访时间为 9.4 个月,安慰剂组(n=201)和 TDF/FTC 组(n=198)的 eGFR 从基线的平均下降斜率分别为-0.88 和-1.53 mL/min/1.73 m/年,斜率差异为 0.65 mL/min/1.73 m/年(p=0.27)。包括两个阶段,389 名参与者开始使用 TDF/FTC 按需治疗,中位随访时间为 19.2 个月,eGFR 从基线下降了-1.14 mL/min/1.73 m/年(p<0.001)。在基线 eGFR≤90 mL/min/1.73 m(p=0.44)、年龄>40 岁(p=0.24)或高血压(p=0.21)的参与者中,eGFR 降低的斜率没有显著差异。考虑到就诊前两个月内服用的药丸数量(每月服用>15 片与≤15 片之间的 eGFR 差异为-0.88 mL/min/1.73 m,p<0.01)或就诊时的血浆替诺福韦浓度(与≤2ng/mL 相比的 eGFR 差异:>2 至≤10ng/mL:-0.98 mL/min/1.73 m,>10 至≤40ng/mL:-1.28 mL/min/1.73 m,>40ng/mL:-1.82 mL/min/1.73 m,p<0.001),存在与 TDF 暴露量之间的剂量反应关系。在 OLE 阶段,有 3 名参与者因 eGFR<60 mL/min/1.73 m 而停止使用 TDF/FTC。没有报告范可尼综合征的病例。
TDF/FTC 按需 PrEP 的肾脏安全性良好。整体的减少和间歇性暴露于 TDF/FTC 可能解释了这种良好的肾脏安全性。