Department of Preventive Medicine Gachon University College of Medicine Incheon Korea.
Artificial Intelligence and Big-Data Convergence Center Gachon University Gil Medical Center Incheon Korea.
J Am Heart Assoc. 2020 Mar 3;9(5):e014840. doi: 10.1161/JAHA.119.014840. Epub 2020 Feb 22.
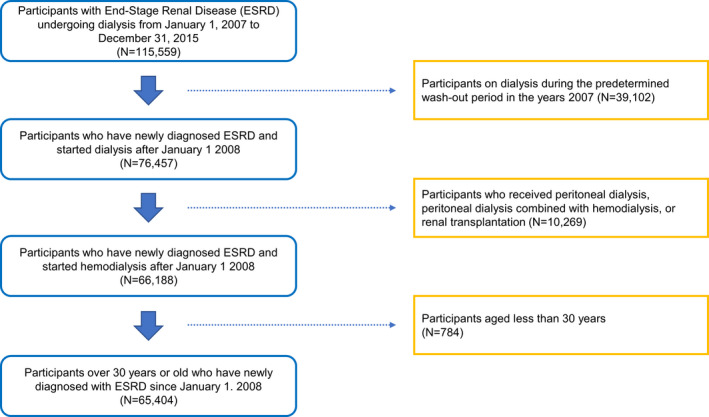
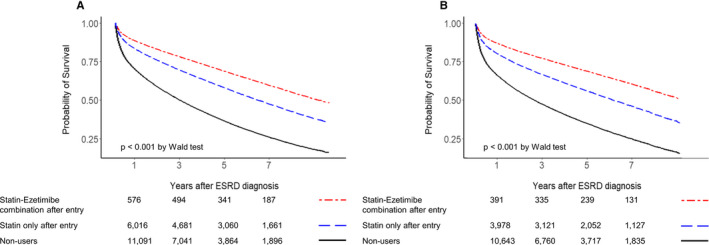
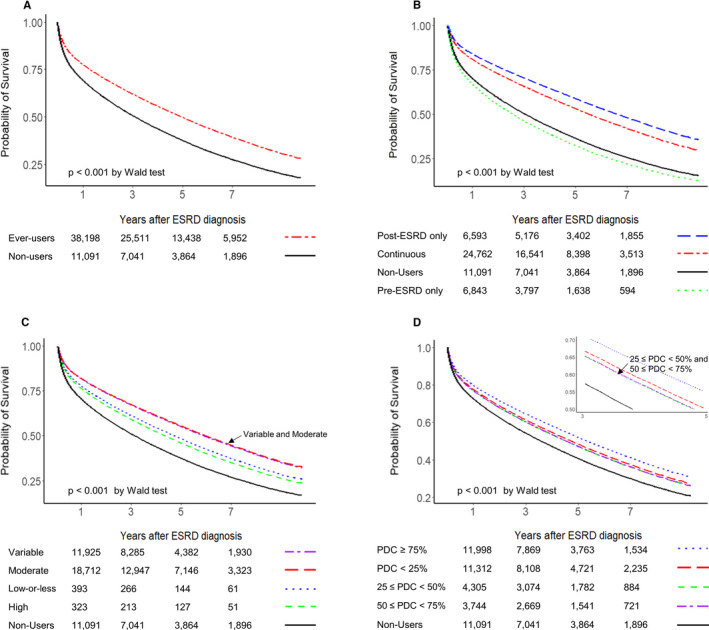
Background Recommendations have not yet been established for statin therapy in patients on maintenance dialysis. In this study, we aimed to evaluate the effects of statin therapy on all-cause mortality in patients undergoing maintenance hemodialysis. Methods and Results This retrospective cohort study analyzed data from adults, aged ≥30 years, who were on maintenance hemodialysis for end-stage renal disease. Data on statin use, along with other clinical information between 2007 and 2017, were extracted from the Health Insurance Review and Assessment Service database in Korea. In total, 65 404 patients were included, and 41 549 (73.2%) patients had received statin therapy for a mean duration of 3.6±2.6 years. Compared with statin nonusers before and after the initiation of hemodialysis (entry), patients who initiated statin therapy after entry and patients who continued statins from the pre-end-stage renal disease to post-end-stage renal disease period had a lower risk of all-cause mortality; the adjusted hazard ratios (95% CIs) were 0.48 (0.47-0.50; <0.001) for post-end-stage renal disease only statin users and 0.59 (0.57-0.60; <0.001) for continuous statin users. However, those discontinuing statins before or at entry showed a higher risk of all-cause mortality. Statin-ezetimibe combinations were associated with better survival benefits than fixed patterns of statin therapy. These results were consistent across various subgroups, including elderly patients aged >75 years, and were maintained even after propensity score matching. Conclusions Our results showed that in adult patients undergoing maintenance hemodialysis, statin therapy, preferably combined with ezetimibe, was associated with a lower risk of all-cause mortality.
对于维持性透析患者,尚未制定他汀类药物治疗的推荐意见。本研究旨在评估他汀类药物治疗对接受维持性血液透析的患者全因死亡率的影响。
本回顾性队列研究分析了来自韩国健康保险审查与评估服务数据库的数据,该数据纳入了年龄≥30 岁、因终末期肾病接受维持性血液透析的成年人。研究提取了 2007 年至 2017 年期间他汀类药物使用情况及其他临床信息。共纳入 65404 例患者,其中 41549 例(73.2%)患者接受他汀类药物治疗,平均治疗时间为 3.6±2.6 年。与开始血液透析前和开始血液透析后(进入期)未使用他汀类药物的患者相比,进入期后开始使用他汀类药物的患者和从终末期肾病前到终末期肾病后持续使用他汀类药物的患者全因死亡率较低;校正后的危险比(95%CI)分别为仅终末期肾病后使用他汀类药物的患者为 0.48(0.47-0.50;<0.001)和持续使用他汀类药物的患者为 0.59(0.57-0.60;<0.001)。然而,那些在进入期之前或进入期内停用他汀类药物的患者全因死亡率较高。与固定模式的他汀类药物治疗相比,他汀类药物联合依折麦布治疗的获益更好。这些结果在包括>75 岁的老年患者在内的各个亚组中一致,并在倾向评分匹配后仍保持不变。
我们的研究结果表明,在接受维持性血液透析的成年患者中,他汀类药物治疗(最好联合依折麦布)与全因死亡率降低相关。