Marcucci Guido, Geyer Susan, Laumann Kristina, Zhao Weiqiang, Bucci Donna, Uy Geoffrey L, Blum William, Eisfeld Ann-Kathrin, Pardee Timothy S, Wang Eunice S, Stock Wendy, Kolitz Jonathan E, Kohlschmidt Jessica, Mrózek Krzysztof, Bloomfield Clara D, Stone Richard M, Larson Richard A
City of Hope Comprehensive Cancer Center, Duarte, CA.
Alliance for Clinical Trials in Oncology Statistics and Data Center, The Ohio State University Comprehensive Cancer Center, Columbus, OH.
Blood Adv. 2020 Feb 25;4(4):696-705. doi: 10.1182/bloodadvances.2019000492.
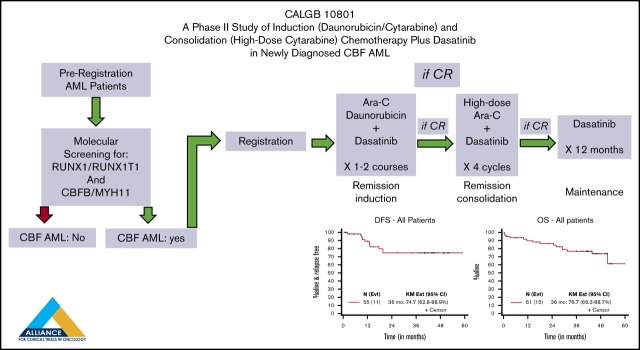
Acute myeloid leukemia (AML) with either t(8;21)(q22;q22) or inv(16)(p13q22)/t(16;16)(p13;q22) is referred to as core binding factor (CBF) AML. Although categorized as favorable risk, long-term survival for these patients is only ∼50% to 60%. Mutated (mut) or overexpressed KIT, a gene encoding a receptor tyrosine kinase, has been found almost exclusively in CBF AML and may increase the risk of disease relapse. We tested the safety and clinical activity of dasatinib, a multi-kinase inhibitor, in combination with chemotherapy. Sixty-one adult patients with AML and CBF fusion transcripts (RUNX1/RUNX1T1 or CBFB/MYH11) were enrolled on Cancer and Leukemia Group B (CALGB) 10801. Patients received cytarabine/daunorubicin induction on days 1 to 7 and oral dasatinib 100 mg/d on days 8 to 21. Upon achieving complete remission, patients received consolidation with high-dose cytarabine followed by dasatinib 100 mg/d on days 6 to 26 for 4 courses, followed by dasatinib 100 mg/d for 12 months. Fifteen (25%) patients were older (aged ≥60 years); 67% were CBFB/MYH11-positive, and 19% harbored KITmut. There were no unexpected or dose-limiting toxicities. Fifty-five (90%) patients achieved complete remission. With a median follow-up of 45 months, only 16% have relapsed. The 3-year disease-free survival and overall survival rates were 75% and 77% (79% and 85% for younger patients [aged <60 years], and 60% and 51% for older patients). Patients with KITmut had comparable outcome to those with wild-type KIT (3-year rates: disease-free survival, 67% vs 75%; overall survival, 73% vs 76%), thereby raising the question of whether dasatinib may overcome the negative impact of these genetic lesions. CALGB 10801 was registered at www.clinicaltrials.gov as #NCT01238211.
伴有t(8;21)(q22;q22)或inv(16)(p13q22)/t(16;16)(p13;q22)的急性髓系白血病(AML)被称为核心结合因子(CBF) AML。尽管被归类为低危,但这些患者的长期生存率仅为50%至60%。编码受体酪氨酸激酶的基因KIT发生突变(mut)或过表达,几乎仅在CBF AML中发现,可能会增加疾病复发风险。我们测试了多激酶抑制剂达沙替尼联合化疗的安全性和临床活性。61例患有AML且有CBF融合转录本(RUNX1/RUNX1T1或CBFB/MYH11)的成年患者入组了癌症与白血病B组(CALGB) 10801研究。患者在第1至7天接受阿糖胞苷/柔红霉素诱导治疗,在第8至21天口服达沙替尼100 mg/d。达到完全缓解后,患者接受大剂量阿糖胞苷巩固治疗,随后在第6至26天接受4个疗程的达沙替尼100 mg/d治疗,之后接受12个月的达沙替尼100 mg/d治疗。15例(25%)患者年龄较大(≥60岁);67%为CBFB/MYH11阳性,19%携带KITmut。未出现意外或剂量限制性毒性。55例(90%)患者达到完全缓解。中位随访45个月,仅16%的患者复发。3年无病生存率和总生存率分别为75%和77%(年龄<60岁的年轻患者分别为79%和85%,年龄较大的患者分别为60%和51%)。携带KITmut的患者与野生型KIT患者的预后相当(3年率:无病生存率,67%对75%;总生存率,73%对76%),从而引发了达沙替尼是否可克服这些基因损伤负面影响的问题。CALGB 10801在www.clinicaltrials.gov上注册,编号为#NCT01238211。