Patel Hima, Yacoub Nour, Mishra Rosalin, White Aaron, Long Yuan, Alanazi Samar, Garrett Joan T
James. L. Winkle College of Pharmacy, University of Cincinnati, Cincinnati, OH 45243, USA.
College of Medicine, Northeast Ohio Medical University, Rootstown, OH 44274, USA.
Cancers (Basel). 2020 Feb 19;12(2):482. doi: 10.3390/cancers12020482.
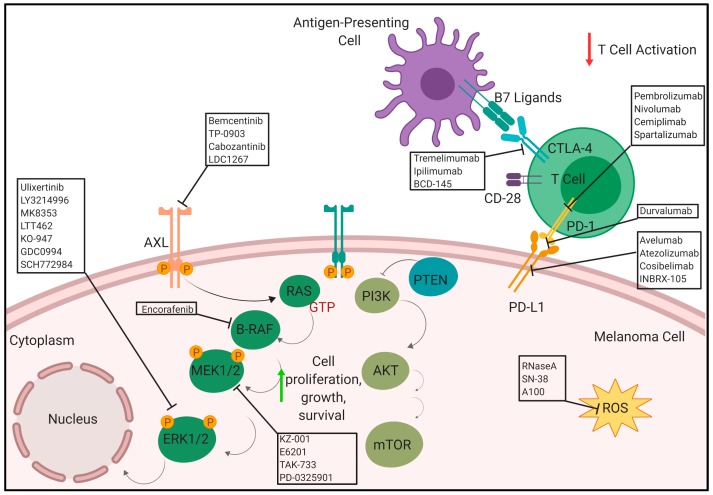
Melanoma is the most lethal form of skin cancer. Melanoma is usually curable with surgery if detected early, however, treatment options for patients with metastatic melanoma are limited and the five-year survival rate for metastatic melanoma had been 15-20% before the advent of immunotherapy. Treatment with immune checkpoint inhibitors has increased long-term survival outcomes in patients with advanced melanoma to as high as 50% although individual response can vary greatly. A mutation within the MAPK pathway leads to uncontrollable growth and ultimately develops into cancer. The most common driver mutation that leads to this characteristic overactivation in the MAPK pathway is the B-RAF mutation. Current combinations of BRAF and MEK inhibitors that have demonstrated improved patient outcomes include dabrafenib with trametinib, vemurafenib with cobimetinib or encorafenib with binimetinib. Treatment with BRAF and MEK inhibitors has met challenges as patient responses began to drop due to the development of resistance to these inhibitors which paved the way for development of immunotherapies and other small molecule inhibitor approaches to address this. Resistance to these inhibitors continues to push the need to expand our understanding of novel mechanisms of resistance associated with treatment therapies. This review focuses on the current landscape of how resistance occurs with the chronic use of BRAF and MEK inhibitors in BRAF-mutant melanoma and progress made in the fields of immunotherapies and other small molecules when used alone or in combination with BRAF and MEK inhibitors to delay or circumvent the onset of resistance for patients with stage III/IV BRAF mutant melanoma.
黑色素瘤是最致命的皮肤癌形式。如果早期发现,黑色素瘤通常可通过手术治愈,然而,转移性黑色素瘤患者的治疗选择有限,在免疫疗法出现之前,转移性黑色素瘤的五年生存率为15%-20%。使用免疫检查点抑制剂进行治疗已将晚期黑色素瘤患者的长期生存结果提高到高达50%,尽管个体反应差异很大。MAPK通路中的突变会导致无法控制的生长并最终发展成癌症。导致MAPK通路出现这种特征性过度激活的最常见驱动突变是B-RAF突变。目前已证明能改善患者预后的BRAF和MEK抑制剂组合包括达拉非尼与曲美替尼、维莫非尼与考比替尼或恩考芬尼与比美替尼。随着患者因对这些抑制剂产生耐药性而反应开始下降,使用BRAF和MEK抑制剂进行治疗遇到了挑战,这为免疫疗法和其他小分子抑制剂方法的开发铺平了道路,以解决这一问题。对这些抑制剂的耐药性持续推动我们需要扩大对与治疗疗法相关的新耐药机制的理解。本综述重点关注BRAF突变型黑色素瘤长期使用BRAF和MEK抑制剂时耐药性产生的现状,以及免疫疗法和其他小分子单独使用或与BRAF和MEK抑制剂联合使用以延迟或规避III/IV期BRAF突变型黑色素瘤患者耐药性发生方面所取得的进展。