Grimm Marc-Oliver, Leucht Katharina, Grünwald Viktor, Foller Susan
Department of Urology, University Hospital Jena, 07747 Jena, Germany.
Interdisciplinary Urology, Western German Tumor Center Essen, Department for Internal Medicine and Urology, University Hospital Essen, 45127 Essen, Germany.
J Clin Med. 2020 Feb 19;9(2):565. doi: 10.3390/jcm9020565.
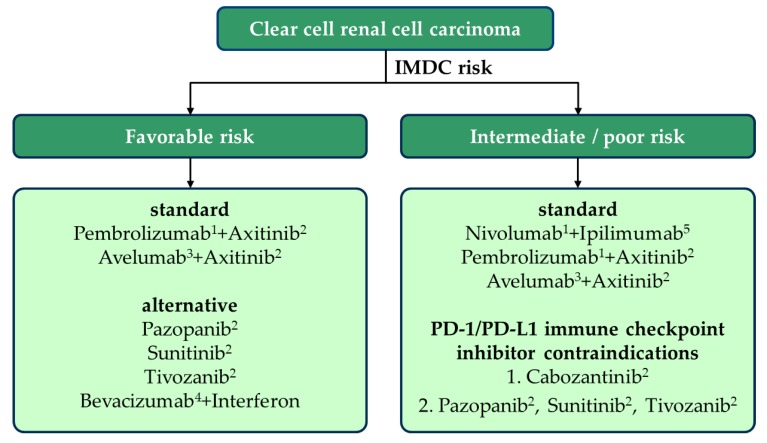
In metastatic renal cell carcinoma (mRCC) the PD-1 immune-checkpoint inhibitor (ICI) Nivolumab became a standard second line treatment option in 2015 based on a significant improvement of overall survival compared to Everolimus. Current pivotal phase 3 studies showed that PD-1 ICI-based combinations were more efficacious than the VEGFR-TKI Sunitinib, a previous standard of care, leading to approval of three new regimens as guideline-recommended first-line treatment. Nivolumab plus Ipilimumab is characterized by a survival advantage, a high rate of complete response and durable remissions in intermediate and poor prognosis patients. Despite frequent immune-mediated side effects, fewer symptoms and a better quality of life were observed compared to Sunitinib. Pembrolizumab or Avelumab plus Axitinib were characterized by an improved progression-free-survival and a high response rate with a low rate of intrinsic resistance. In addition, Pembrolizumab plus Axitinib reached a significant survival benefit. The side effect profile is driven by the chronic toxicity of Axitinib, but there is additional risk of immune-mediated side effects of the PD-1/PD-L1 ICIs. The quality of life data published so far do not suggest any improvement regarding patient-reported outcomes compared to the previous standard Sunitinib. The PD-1/PD-L1 ICIs thus form the backbone of the first-line therapy of mRCC.
在转移性肾细胞癌(mRCC)中,基于与依维莫司相比总体生存期有显著改善,程序性死亡受体1(PD-1)免疫检查点抑制剂(ICI)纳武单抗在2015年成为标准的二线治疗选择。目前的关键3期研究表明,基于PD-1 ICI的联合治疗比先前的标准治疗药物血管内皮生长因子受体酪氨酸激酶抑制剂(VEGFR-TKI)舒尼替尼更有效,从而使三种新方案获批成为指南推荐的一线治疗方案。纳武单抗加伊匹单抗的特点是在中、低预后患者中具有生存优势、高完全缓解率和持久缓解。尽管免疫介导的副作用频繁,但与舒尼替尼相比,观察到的症状更少,生活质量更高。帕博利珠单抗或阿维鲁单抗加阿昔替尼的特点是无进展生存期改善、缓解率高且内在耐药率低。此外,帕博利珠单抗加阿昔替尼具有显著的生存获益。副作用特征由阿昔替尼的慢性毒性驱动,但PD-1/程序性死亡受体配体1(PD-L1)ICI存在免疫介导副作用的额外风险。与先前的标准治疗药物舒尼替尼相比,迄今为止公布的生活质量数据并未显示患者报告结局有任何改善。因此,PD-1/PD-L1 ICI构成了mRCC一线治疗的基础。