Puliani Giulia, Sesti Franz, Feola Tiziana, Di Leo Nicola, Polti Giorgia, Verrico Monica, Modica Roberta, Colao Annamaria, Lenzi Andrea, Isidori Andrea M, Cantisani Vito, Giannetta Elisa, Faggiano Antongiulio
Department of Experimental Medicine, Sapienza University of Rome, 00161 Rome, Italy.
Department of Radiological, Pathological and Oncological Sciences, Sapienza University of Rome, 00161 Rome, Italy.
J Clin Med. 2020 Feb 21;9(2):588. doi: 10.3390/jcm9020588.
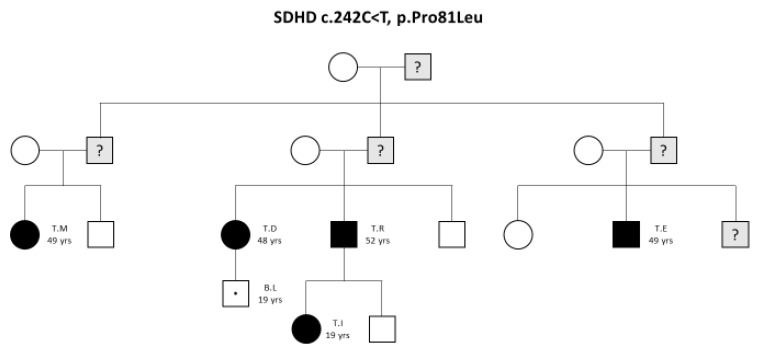
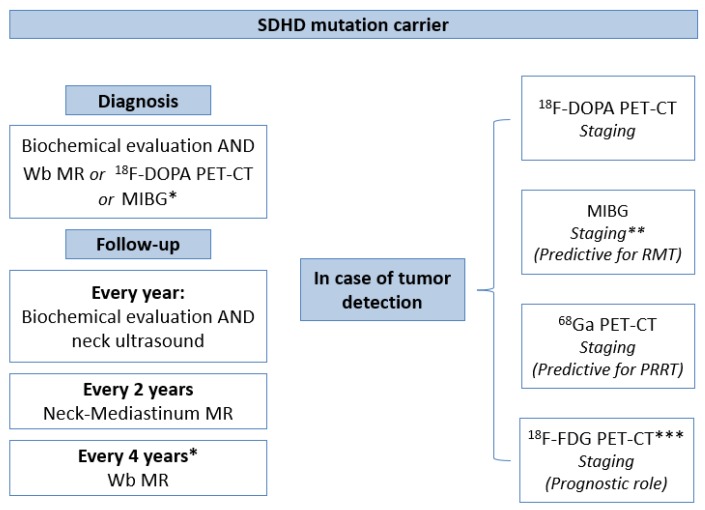
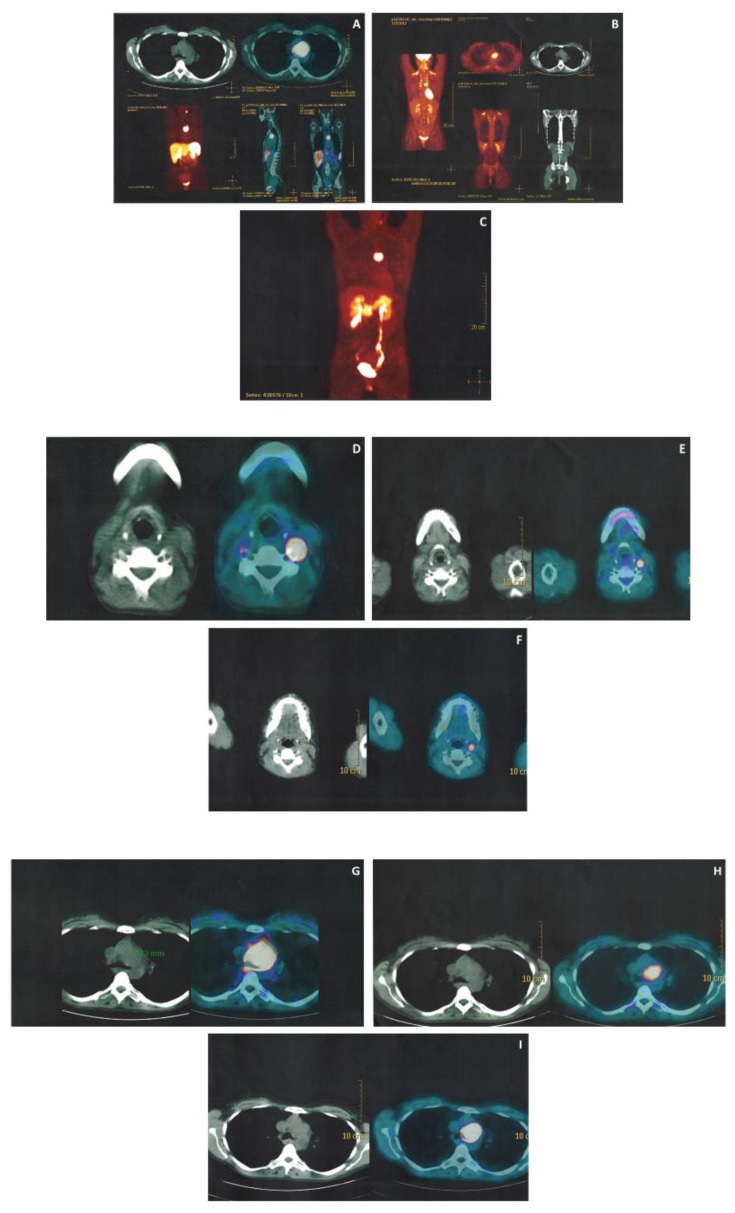
Head and neck paragangliomas are the most common clinical features of familial paraganglioma syndrome type 1 caused by succinate dehydrogenase complex subunit D (SDHD) mutation. The clinical management of this syndrome is still unclear. In this study we propose a diagnostic algorithm for SDHD mutation carriers based on our family case series and literature review. After genetic diagnosis, first evaluation should include biochemical examination and whole-body imaging. In case of lesion detection, nuclear medicine examination is required for staging and tumor characterization. The study summarizes the diagnostic accuracy of different functional imaging techniques in SDHD mutation carriers. 18F-3,4-dihydroxyphenylalanine (18F-DOPA) positron emission tomography (PET)-computed tomography (CT) is considered the gold standard. If it is not available, 123I-Metaiodobenzylguanidine (MIBG) could be used also for predicting response to radiometabolic therapy. 18F-fluoro-2-deoxy-D-glucose (18F-FDG) PET-CT has a prognostic role since high uptake identifies more aggressive cases. Finally, 68Ga-peptides PET-CT is a promising diagnostic technique, demonstrating the best diagnostic accuracy in our and in other published case series, even if this finding still needs to be confirmed in larger studies. Periodic follow-up should consist of annual biochemical and ultrasonographic screening and biannual magnetic resonance examination to identify biochemical silent tumors early.
头颈部副神经节瘤是由琥珀酸脱氢酶复合物亚基D(SDHD)突变引起的1型家族性副神经节瘤综合征最常见的临床特征。该综合征的临床管理仍不明确。在本研究中,我们基于我们的家族病例系列和文献综述,提出了一种针对SDHD突变携带者的诊断算法。基因诊断后,首次评估应包括生化检查和全身成像。如检测到病变,则需要进行核医学检查以进行分期和肿瘤特征描述。本研究总结了不同功能成像技术在SDHD突变携带者中的诊断准确性。18F-3,4-二羟基苯丙氨酸(18F-DOPA)正电子发射断层扫描(PET)-计算机断层扫描(CT)被认为是金标准。如果无法进行该检查,123I-间碘苄胍(MIBG)也可用于预测对放射代谢治疗的反应。18F-氟-2-脱氧-D-葡萄糖(18F-FDG)PET-CT具有预后作用,因为高摄取表明病情更具侵袭性。最后,68Ga-肽PET-CT是一种有前景的诊断技术,在我们的病例系列和其他已发表的病例系列中显示出最佳诊断准确性,尽管这一发现仍需在更大规模的研究中得到证实。定期随访应包括每年的生化和超声筛查以及每半年的磁共振检查,以便早期发现生化隐匿性肿瘤。