Ahn Kye Taek, Oh Jin Kyung, Seong Seok Woo, Jin Seon Ah, Lee Jae Hwan, Choi Si Wan, Jeong Myung Ho, Chae Shung Chull, Kim Young Jo, Kim Chong Jin, Kim Hyo Soo, Cho Myeong Chan, Gwon Hyeon Cheol, Jeong Jin Ok, Seong In Whan
Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University College of Medicine, Daejeon, Korea.
Division of Cardiology, Department of Internal Medicine, Chonnam National University Hospital, Gwangju, Korea.
Korean Circ J. 2020 Mar;50(3):220-233. doi: 10.4070/kcj.2019.0176.
Although complete revascularization is known superior to incomplete revascularization in ST elevation myocardial infarction (STEMI) patients with multi-vessel coronary artery disease (MVCD), there are no definite instructions on the optimal timing of non-culprit lesions percutaneous coronary intervention (PCI). We compared 1-year clinical outcomes between 2 different complete multi-vessel revascularization strategies.
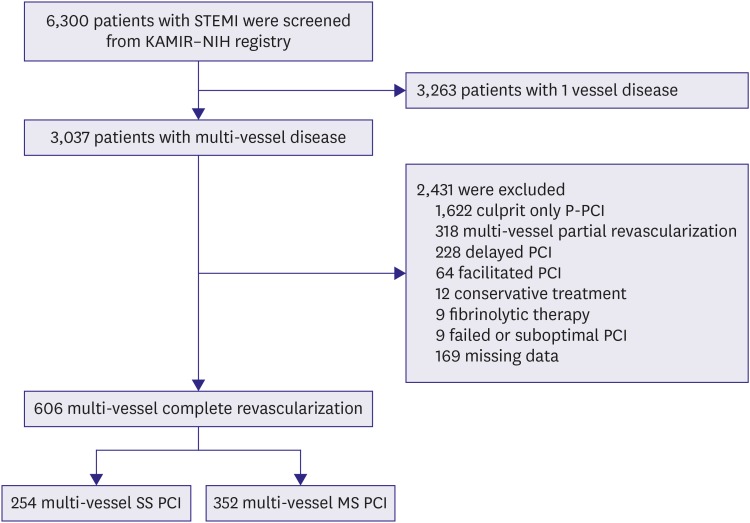
From the Korea Acute Myocardial Infarction Registry-National Institute of Health, 606 patients with STEMI and MVCD who underwent complete revascularization were enrolled from November 2011 to December 2015. The patients were assigned to multi-vessel single-staged PCI (SS PCI) group (n=254) or multi-vessel multi-staged PCI (MS PCI) group (n=352). Propensity score matched 1-year clinical outcomes were compared between the groups.
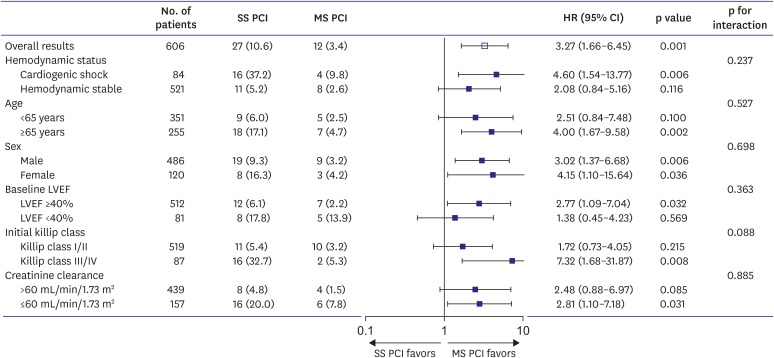
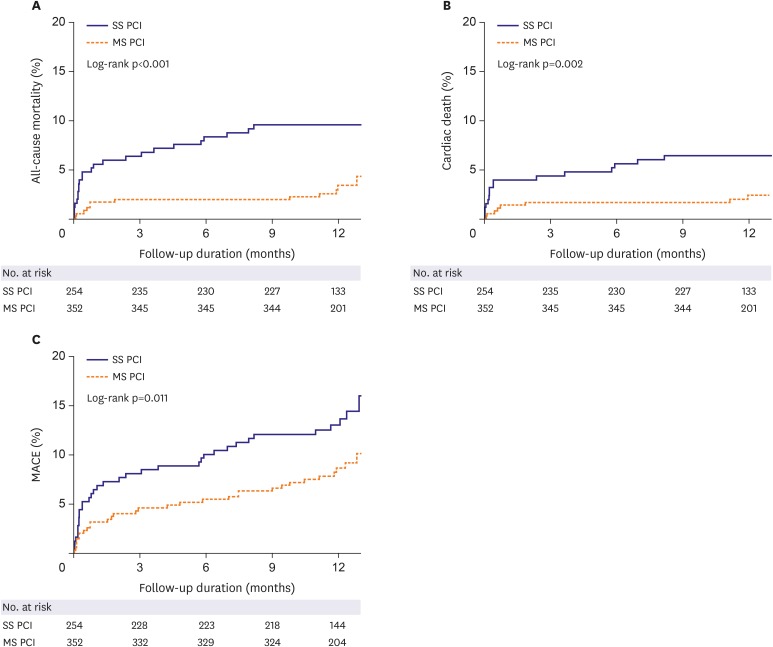
At one year, MS PCI showed a significantly lower rate of all-cause mortality (hazard ratio [HR], 0.42; 95% confidential interval [CI], 0.19-0.92; p=0.030) compared with SS PCI. In subgroup analysis, all-cause mortality increased in SS PCI with cardiogenic shock (HR, 4.60; 95% CI, 1.54-13.77; p=0.006), age ≥65 years (HR, 4.00; 95% CI, 1.67-9.58, p=0.002), Killip class III/IV (HR, 7.32; 95% CI, 1.68-31.87; p=0.008), and creatinine clearance ≤60 mL/min (HR, 2.81; 95% CI, 1.10-7.18; p=0.031). After propensity score-matching, MS PCI showed a significantly lower risk of major adverse cardiovascular event than SS PCI.
SS PCI was associated with worse clinical outcomes compared with MS PCI. MS PCI for non-infarct-related artery could be a better option for patients with STEMI and MVCD, especially high-risk patients.
虽然在患有多支冠状动脉疾病(MVCD)的ST段抬高型心肌梗死(STEMI)患者中,完全血运重建优于不完全血运重建,但对于非罪犯病变经皮冠状动脉介入治疗(PCI)的最佳时机尚无明确指导。我们比较了两种不同的完全多支血管血运重建策略的1年临床结局。
从韩国急性心肌梗死注册研究-国立卫生研究院中,选取2011年11月至2015年12月期间接受完全血运重建的606例STEMI和MVCD患者。将患者分为多支血管单阶段PCI(SS PCI)组(n = 254)或多支血管多阶段PCI(MS PCI)组(n = 352)。比较两组倾向评分匹配后的1年临床结局。
1年时,与SS PCI相比,MS PCI的全因死亡率显著更低(风险比[HR],0.42;95%可信区间[CI],0.19 - 0.92;p = 0.030)。在亚组分析中,SS PCI组中的心源性休克(HR,4.60;95% CI,1.54 - 13.77;p = 0.006)、年龄≥65岁(HR,4.00;95% CI,1.67 - 9.58,p = 0.002)、Killip分级III/IV级(HR,7.32;95% CI,1.68 - 31.87;p = 0.008)以及肌酐清除率≤60 mL/min(HR,2.81;95% CI,1.10 - 7.18;p = 0.031)患者的全因死亡率增加。倾向评分匹配后,MS PCI的主要不良心血管事件风险显著低于SS PCI。
与MS PCI相比,SS PCI与更差的临床结局相关。对于STEMI和MVCD患者,尤其是高危患者,对非梗死相关动脉进行MS PCI可能是更好的选择。