Formerly Office of the Clinical Director, Intramural Research Program, National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, Bethesda, Maryland.
WakeMed Physician Practices, Raleigh, North Carolina.
JAMA Netw Open. 2020 Feb 5;3(2):e200032. doi: 10.1001/jamanetworkopen.2020.0032.
Immune checkpoint inhibitors (ICIs) have transformed the treatment paradigm for an ever-increasing number of cancers. However, their use has also led to the emergence of immune-related adverse events, such as ICI-induced inflammatory arthritis. A reproducible, reliable, and accessible modality is needed to assess and distinguish early ICI-induced inflammatory arthritis and help in management. Magnetic resonance imaging (MRI) of joints may be helpful for early diagnosis, guiding therapeutic decision-making, and identifying patients at high risk for erosive disease.
To assess the role of MRI of joints in patients with ICI-induced inflammatory arthritis.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective case series included patients enrolled at the National Institutes of Health Clinical Center in Bethesda, Maryland. Patients were evaluated by the rheumatology consultation service between December 27, 2016, and May 28, 2019. A retrospective health record review was performed to determine demographic characteristics, clinical characteristics of inflammatory arthritis and malignant tumors, and imaging findings. Inclusion criteria were patients who were enrolled on various institutional review board-approved protocols of ICIs, developed joint-related symptoms, and had MRI data for at least 1 joint. Data were analyzed from June 1, 2019, to September 1, 2019.
Undergoing MRI of at least 1 joint.
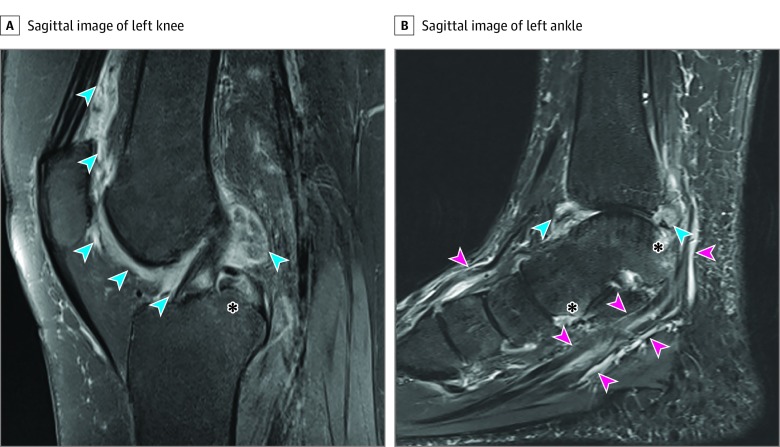
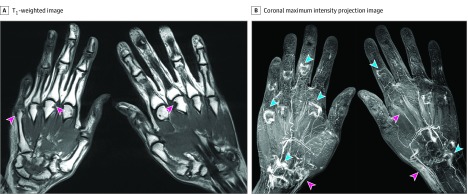
All MRIs were reviewed for synovitis, tenosynovitis, bone marrow edema, and soft tissue conditions.
A total of 8 patients (mean [SD] age, 58.8 [5.2] years; 6 women and 2 men) between the ages of 50 and 65 years who were undergoing ICI therapy for a variety of malignant tumors were included in this study. Only 1 patient was receiving combined ICI therapy. The results of 13 separate MRI examinations were reviewed. The most commonly performed MRIs were of the hands and wrists (9 MRIs), followed by knee examinations (3 MRIs). Tenosynovitis and synovitis were frequently seen in the hands and wrists. Bone marrow edema and erosions were also found in 3 patients, suggesting early damage. In larger joints (ie, knees and ankles), joint effusions and synovial thickening were characteristic. Most patients (5 patients) were treated with corticosteroids and had good responses. In patients with high-risk features on MRI imaging (eg, bone marrow edema, erosions), disease-modifying antirheumatic drug therapy was also discussed as a treatment option.
These findings suggest that advanced imaging may help to distinguish ICI-induced inflammatory arthritis from other causes of joint pain, aid in identifying patients at increased risk of joint damage, and provide utility in monitoring inflammatory arthritis treatment response in patients receiving ICI therapy.
免疫检查点抑制剂(ICIs)已经改变了越来越多癌症的治疗模式。然而,它们的使用也导致了免疫相关的不良反应的出现,如ICI 诱导的炎性关节炎。需要一种可重复、可靠和易于获得的方式来评估和区分早期 ICI 诱导的炎性关节炎,并有助于管理。关节磁共振成像(MRI)可能有助于早期诊断、指导治疗决策,并识别出有侵蚀性疾病高风险的患者。
评估关节 MRI 在 ICI 诱导的炎性关节炎患者中的作用。
设计、地点和参与者:本回顾性病例系列研究纳入了在马里兰州贝塞斯达市美国国立卫生研究院临床中心就诊的患者。这些患者于 2016 年 12 月 27 日至 2019 年 5 月 28 日期间接受了风湿病咨询服务的评估。对健康记录进行了回顾性分析,以确定患者的人口统计学特征、炎性关节炎和恶性肿瘤的临床特征以及影像学发现。纳入标准为:患者入组了各种机构审查委员会批准的 ICI 试验,出现关节相关症状,并且至少有 1 个关节的 MRI 数据。数据分析于 2019 年 6 月 1 日至 2019 年 9 月 1 日进行。
至少进行 1 次关节 MRI。
所有 MRI 均评估了滑膜炎、腱鞘炎、骨髓水肿和软组织情况。
本研究共纳入 8 例(平均[标准差]年龄,58.8[5.2]岁;6 名女性和 2 名男性)年龄在 50 岁至 65 岁之间的患者,他们正在接受各种恶性肿瘤的 ICI 治疗。仅有 1 例患者接受联合 ICI 治疗。共回顾了 13 次单独的 MRI 检查结果。最常进行的 MRI 是手部和腕部(9 次 MRI),其次是膝关节检查(3 次 MRI)。手部常出现腱鞘炎和滑膜炎。3 例患者还发现骨髓水肿和侵蚀,提示早期损伤。在较大的关节(即膝关节和踝关节)中,关节积液和滑膜增厚是特征性表现。大多数患者(5 例)接受了皮质类固醇治疗,反应良好。在 MRI 影像学上有高风险特征的患者(例如骨髓水肿、侵蚀),也讨论了使用疾病修饰抗风湿药物治疗作为一种治疗选择。
这些发现表明,高级影像学可能有助于区分 ICI 诱导的炎性关节炎与其他关节疼痛的原因,有助于识别关节损伤风险增加的患者,并为接受 ICI 治疗的患者监测炎性关节炎治疗反应提供依据。