Department of Surgery, Amsterdam UMC (location AMC), University of Amsterdam, Amsterdam, The Netherlands.
Department of Surgery, Erasmus Medical Center, Rotterdam, The Netherlands.
Ann Surg Oncol. 2020 Jul;27(7):2311-2318. doi: 10.1245/s10434-020-08258-3. Epub 2020 Feb 26.
Preoperative portal vein embolization (PVE) is frequently used to improve future liver remnant volume (FLRV) and to reduce the risk of liver failure after major liver resection.
This paper aimed to assess postoperative outcomes after PVE and resection for suspected perihilar cholangiocarcinoma (PHC) in an international, multicentric cohort.
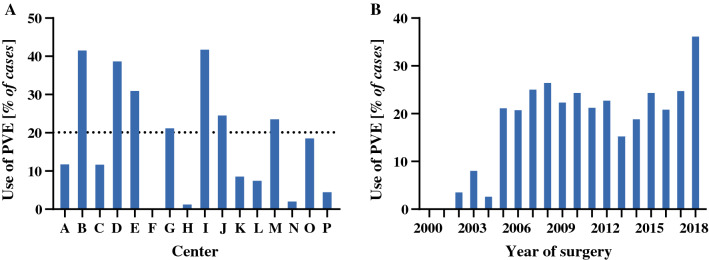
Patients undergoing resection for suspected PHC across 20 centers worldwide, from the year 2000, were included. Liver failure, biliary leakage, and hemorrhage were classified according to the respective International Study Group of Liver Surgery criteria. Using propensity scoring, two equal cohorts were generated using matching parameters, i.e. age, sex, American Society of Anesthesiologists classification, jaundice, type of biliary drainage, baseline FLRV, resection type, and portal vein resection.
A total of 1667 patients were treated for suspected PHC during the study period. In 298 patients who underwent preoperative PVE, the overall incidence of liver failure and 90-day mortality was 27% and 18%, respectively, as opposed to 14% and 12%, respectively, in patients without PVE (p < 0.001 and p = 0.005). After propensity score matching, 98 patients were enrolled in each cohort, resulting in similar baseline and operative characteristics. Liver failure was lower in the PVE group (8% vs. 36%, p < 0.001), as was biliary leakage (10% vs. 35%, p < 0.01), intra-abdominal abscesses (19% vs. 34%, p = 0.01), and 90-day mortality (7% vs. 18%, p = 0.03).
PVE before major liver resection for PHC is associated with a lower incidence of liver failure, biliary leakage, abscess formation, and mortality. These results demonstrate the importance of PVE as an integral component in the surgical treatment of PHC.
术前门静脉栓塞术(PVE)常用于增加未来肝脏剩余体积(FLRV)并降低大肝切除术后肝功能衰竭的风险。
本研究旨在评估国际多中心队列中 PVE 联合切除术治疗可疑肝门部胆管癌(PHC)的术后结局。
纳入 2000 年以来全球 20 个中心接受可疑 PHC 切除术的患者。肝功能衰竭、胆漏和出血根据各自的国际肝脏外科研究组(ISGLS)标准进行分类。采用倾向评分匹配方法,使用匹配参数(年龄、性别、美国麻醉医师协会分类、黄疸、胆道引流类型、基线 FLRV、切除类型和门静脉切除)生成两组相等的队列。
研究期间共治疗 1667 例疑似 PHC 患者。在接受术前 PVE 的 298 例患者中,肝功能衰竭和 90 天死亡率的总发生率分别为 27%和 18%,而未行 PVE 的患者分别为 14%和 12%(p<0.001 和 p=0.005)。经倾向评分匹配后,每组纳入 98 例患者,两组基线和手术特征相似。PVE 组肝功能衰竭发生率较低(8% vs. 36%,p<0.001),胆漏发生率较低(10% vs. 35%,p<0.01),腹腔脓肿发生率较低(19% vs. 34%,p=0.01),90 天死亡率较低(7% vs. 18%,p=0.03)。
PHC 患者行大肝切除术前 PVE 可降低肝功能衰竭、胆漏、脓肿形成和死亡率的发生率。这些结果表明,PVE 是 PHC 外科治疗不可或缺的一部分。