Division of Critical Care Medicine, Department of Pediatrics, University of Michigan, Ann Arbor, MI.
Susan B Meister Child Health Evaluation and Research Center, Department of Pediatrics, University of Michigan, Ann Arbor, MI.
Crit Care Med. 2020 May;48(5):725-731. doi: 10.1097/CCM.0000000000004272.
Severe sepsis is a significant cause of healthcare utilization and morbidity among pediatric patients. However, little is known about how commonly survivors acquire new medical devices during pediatric severe sepsis hospitalization. We sought to determine the rate of new device acquisition (specifically, tracheostomy placement, gastrostomy tube placement, vascular access devices, ostomy procedures, and amputation) among children surviving hospitalizations with severe sepsis. For contextualization, we compare this to rates of new device acquisition among three comparison cohorts: 1) survivors of all-cause pediatric hospitalizations; 2) matched survivors of nonsepsis infection hospitalizations; and 3) matched survivors of all-cause nonsepsis hospitalization with similar organ dysfunction.
Observational cohort study.
Nationwide Readmission Database (2016), including all-payer hospitalizations from 27 states.
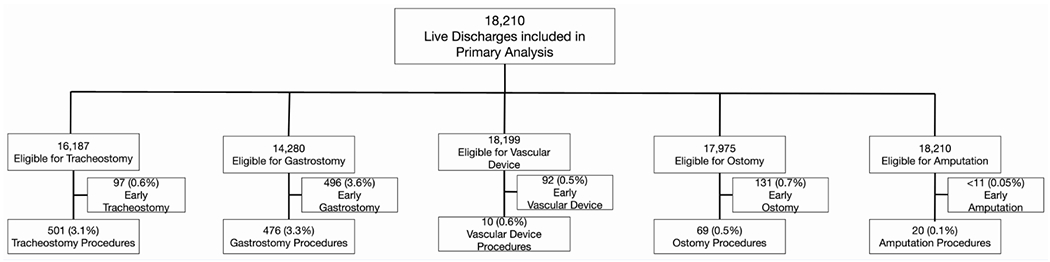
Eighteen-thousand two-hundred ten pediatric severe sepsis hospitalizations; 532,738 all-cause pediatric hospitalizations; 16,173 age- and sex-matched nonsepsis infection hospitalizations; 15,025 organ dysfunction matched all-cause nonsepsis hospitalizations; and all with live discharge.
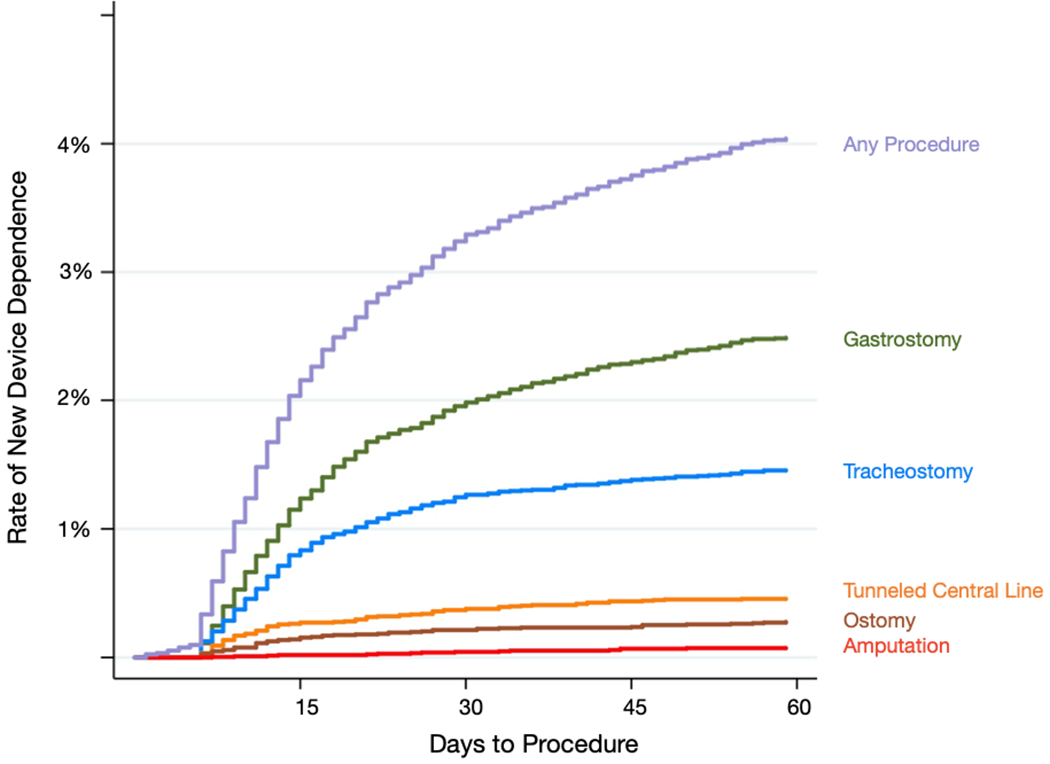
Among 18,210 pediatric severe sepsis hospitalizations, 1,024 (5.6%) underwent device placement. Specifically, 3.5% had new gastrostomy, 3.1% new tracheostomy, 0.6% new vascular access devices, 0.4% new ostomy procedures, and 0.1% amputations. One-hundred forty hospitalizations (0.8%) included two or more new devices. After applying the Nationwide Readmissions Database sampling weights, there were 55,624 pediatric severe sepsis hospitalizations and 1,585,194 all-cause nonsepsis hospitalizations with live discharge in 2016. Compared to all-cause pediatric hospitalizations, severe sepsis hospitalizations were eight-fold more likely to involve new device acquisition (6.4% vs 0.8%; p < 0.001). New device acquisition was also higher in severe sepsis hospitalizations compared with matched nonsepsis infection hospitalizations (5.1% vs 1.2%; p < 0.01) and matched all-cause hospitalizations with similar organ dysfunction (4.7% vs 2.8%; p < 0.001).
In this nationwide, all-payer cohort of U.S. pediatric severe sepsis hospitalizations, one in 20 children surviving severe sepsis experienced new device acquisition. The procedure rate was nearly eight-fold higher than all-cause, nonsepsis pediatric hospitalizations, and four-fold higher than matched nonsepsis infection hospitalizations.
严重脓毒症是儿科患者医疗利用和发病的重要原因。然而,对于脓毒症存活患儿在住院期间获得新医疗器械的频率知之甚少。我们旨在确定严重脓毒症住院患儿中获得新医疗器械(具体为气管造口术、胃造口术、血管通路装置、造口术和截肢)的比例。为了进行背景比较,我们将此比例与以下三个对照组的新医疗器械获得率进行比较:1)所有原因儿科住院的存活患儿;2)匹配的非脓毒症感染住院的存活患儿;3)匹配的所有原因非脓毒症住院且器官功能障碍相似的存活患儿。
观察性队列研究。
全国再入院数据库(2016 年),包括来自 27 个州的全支付医院住院患者。
18210 例儿科严重脓毒症住院患者;532738 例所有原因儿科住院患者;16173 例年龄和性别匹配的非脓毒症感染住院患者;15025 例器官功能障碍匹配的所有原因非脓毒症住院患者,且均存活出院。
在 18210 例儿科严重脓毒症住院患者中,有 1024 例(5.6%)进行了器械放置。具体来说,3.5%的患者接受了新的胃造口术,3.1%的患者接受了新的气管造口术,0.6%的患者接受了新的血管通路装置,0.4%的患者接受了新的造口术,0.1%的患者接受了截肢术。140 例(0.8%)住院患者有两种或更多新器械。应用全国再入院数据库抽样权重后,2016 年有 55624 例儿科严重脓毒症住院患者和 1585194 例所有原因非脓毒症住院患者存活出院。与所有原因儿科住院患者相比,严重脓毒症住院患者发生新器械获取的可能性高 8 倍(6.4%比 0.8%;p<0.001)。严重脓毒症住院患者的新器械获取率也高于匹配的非脓毒症感染住院患者(5.1%比 1.2%;p<0.01)和匹配的所有原因器官功能障碍相似的住院患者(4.7%比 2.8%;p<0.001)。
在这项针对美国儿科严重脓毒症住院患者的全国性、全支付队列研究中,每 20 名存活的严重脓毒症患儿中就有 1 名经历了新的器械获取。该手术率几乎是所有原因非脓毒症儿科住院患者的 8 倍,是匹配的非脓毒症感染住院患者的 4 倍。