Avenir Health, Glastonbury, CT, USA.
The Palladium Group, Washington, DC, USA.
J Int AIDS Soc. 2020 Feb;23(2):e25451. doi: 10.1002/jia2.25451.
Oral pre-exposure prophylaxis (PrEP) provision is a priority intervention for high HIV prevalence settings and populations at substantial risk of HIV acquisition. This mathematical modelling analysis estimated the impact, cost and cost-effectiveness of scaling up oral PrEP in 13 countries.
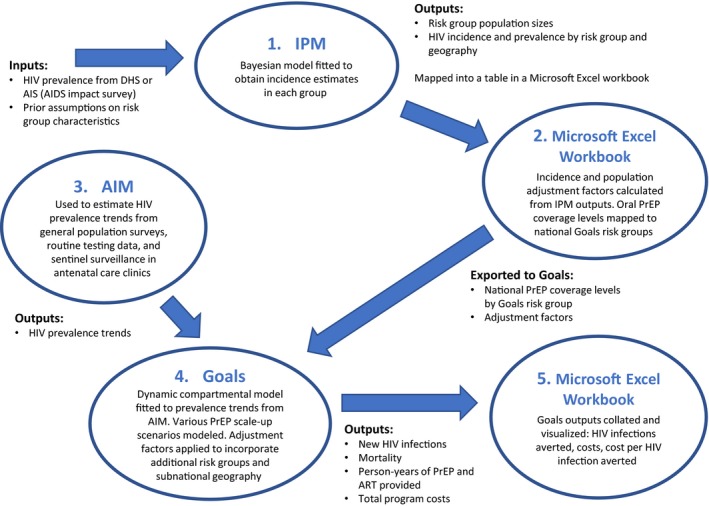
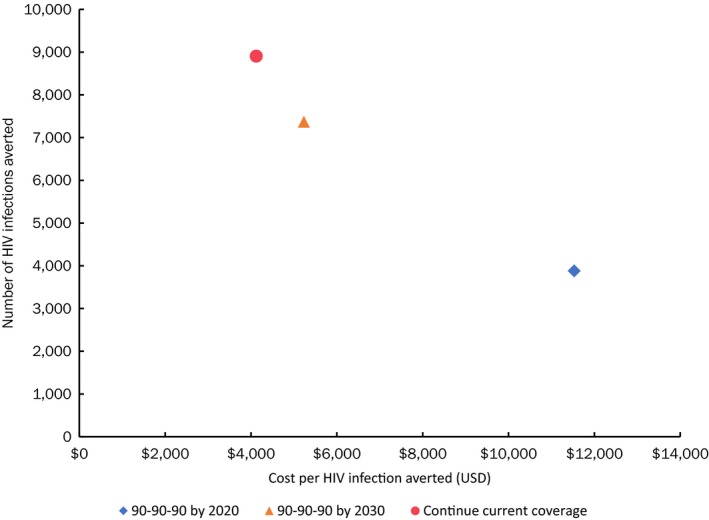
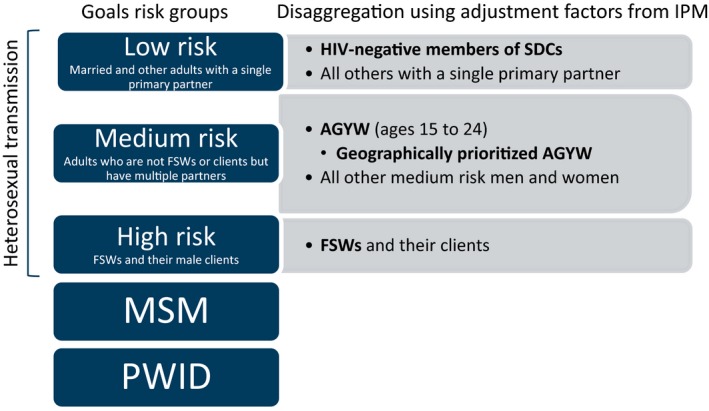
We projected the impact and cost-effectiveness of oral PrEP between 2018 and 2030 using a combination of the Incidence Patterns Model and the Goals model. We created four PrEP rollout scenarios involving three priority populations-female sex workers (FSWs), serodiscordant couples (SDCs) and adolescent girls and young women (AGYW)-both with and without geographic prioritization. We applied the model to 13 countries (Eswatini, Ethiopia, Haiti, Kenya, Lesotho, Mozambique, Namibia, Nigeria, Tanzania, Uganda, Zambia and Zimbabwe). The base case assumed achievement of the Joint United Nations Programme on HIV/AIDS 90-90-90 antiretroviral therapy targets, 90% male circumcision coverage by 2020 and 90% efficacy and adherence levels for oral PrEP.
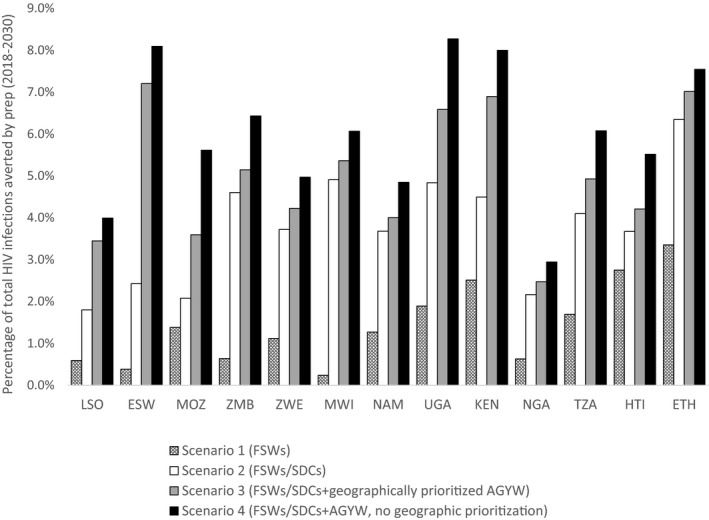
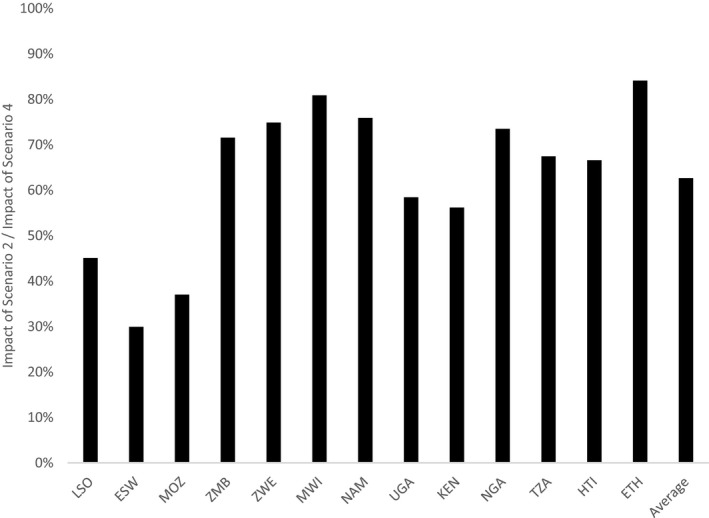
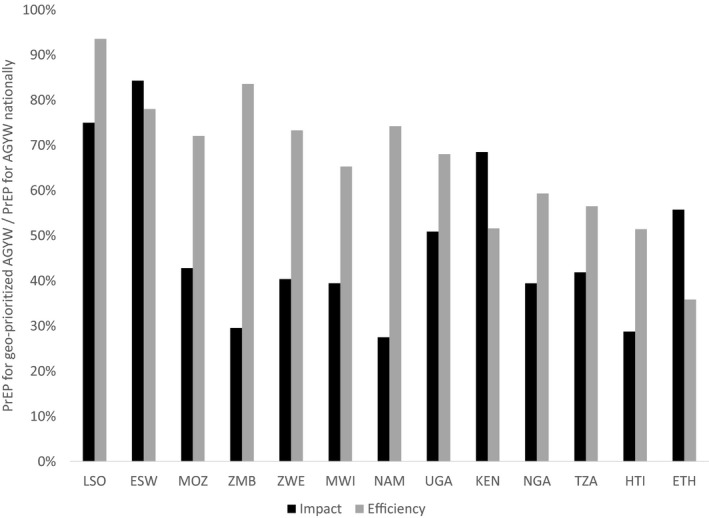
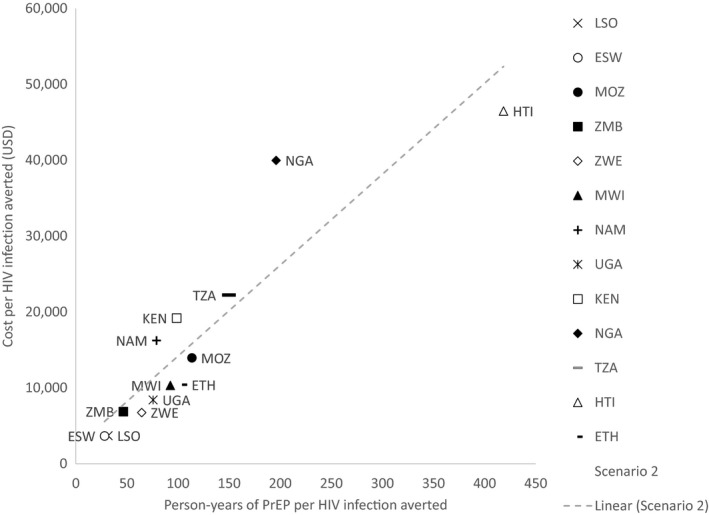
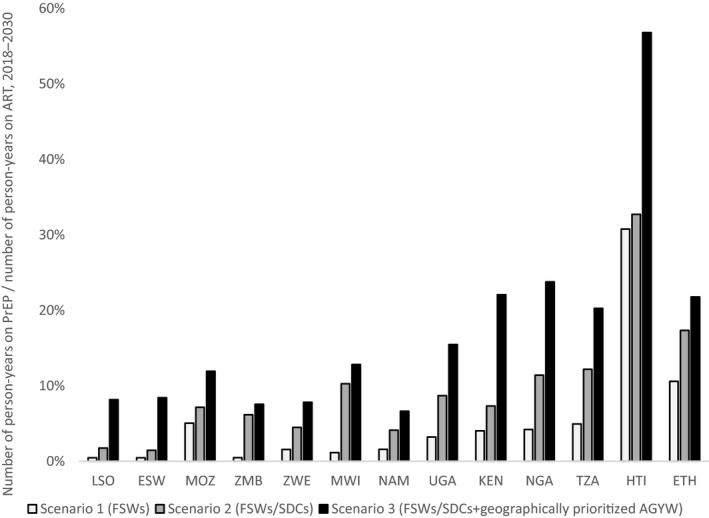
In the scenarios we examined, oral PrEP averted 3% to 8% of HIV infections across the 13 countries between 2018 and 2030. For all but three countries, more than 50% of the HIV infections averted by oral PrEP in the scenarios we examined could be obtained by rollout to FSWs and SDCs alone. For several countries, expanding oral PrEP to include medium-risk AGYW in all regions greatly increased the impact. The efficiency and impact benefits of geographic prioritization of rollout to AGYW varied across countries. Variations in cost-effectiveness across countries reflected differences in HIV incidence and expected variations in unit cost. For most countries, rolling out oral PrEP to FSWs, SDCs and geographically prioritized AGYW was not projected to have a substantial impact on the supply chain for antiretroviral drugs.
These modelling results can inform prioritization, target-setting and other decisions related to oral PrEP scale-up within combination prevention programmes. We caution against extensive use given limitations in cost data and implementation approaches. This analysis highlights some of the immediate challenges facing countries-for example, trade-offs between overall impact and cost-effectiveness-and emphasizes the need to improve data availability and risk assessment tools to help countries make informed decisions.
口腔暴露前预防(PrEP)的提供是高 HIV 流行地区和具有大量 HIV 感染风险人群的优先干预措施。本数学建模分析估计了在 13 个国家扩大口腔 PrEP 的影响、成本和成本效益。
我们使用 Incidence Patterns Model 和 Goals model 相结合的方法,预测了 2018 年至 2030 年期间口腔 PrEP 的影响和成本效益。我们创建了四个 PrEP 推出场景,涉及三个优先人群-女性性工作者(FSWs)、性伴侣不一致的夫妇(SDCs)和青少年女孩和年轻妇女(AGYW)-以及是否具有地理优先级。我们将模型应用于 13 个国家(斯威士兰、埃塞俄比亚、海地、肯尼亚、莱索托、莫桑比克、纳米比亚、尼日利亚、坦桑尼亚、乌干达、赞比亚和津巴布韦)。基础情况假设实现联合国艾滋病规划署 90-90-90 抗逆转录病毒治疗目标,2020 年男性割礼覆盖率达到 90%,口腔 PrEP 的疗效和依从率达到 90%。
在我们研究的场景中,2018 年至 2030 年期间,口腔 PrEP 在 13 个国家中预防了 3%至 8%的 HIV 感染。除了三个国家之外,我们研究的场景中口腔 PrEP 预防的 HIV 感染中,超过 50%可以通过向 FSWs 和 SDCs 单独推出来获得。对于一些国家来说,将口腔 PrEP 扩大到所有地区的中风险 AGYW,可以大大增加其影响。在各国,扩大口腔 PrEP 的地理优先次序,向 AGYW 推出,在提高效率和影响方面存在差异。各国之间的成本效益差异反映了 HIV 发病率的差异和单位成本的预期变化。对于大多数国家来说,向 FSWs、SDCs 和地理优先的 AGYW 推出口腔 PrEP,预计不会对抗逆转录病毒药物的供应链产生重大影响。
这些建模结果可以为组合预防方案中的口腔 PrEP 扩大提供优先事项、目标设定和其他决策方面的信息。我们警告说,鉴于成本数据和实施方法的局限性,不应广泛使用。本分析突出了一些国家面临的直接挑战,例如总体影响和成本效益之间的权衡,并强调需要改善数据可用性和风险评估工具,以帮助国家做出明智的决策。