Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Front Immunol. 2020 Feb 7;11:149. doi: 10.3389/fimmu.2020.00149. eCollection 2020.
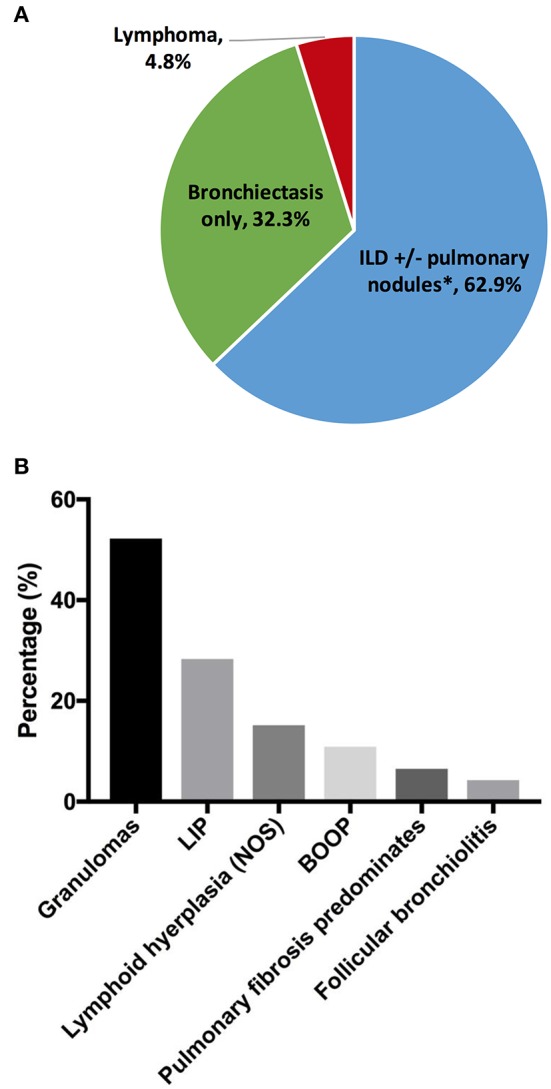
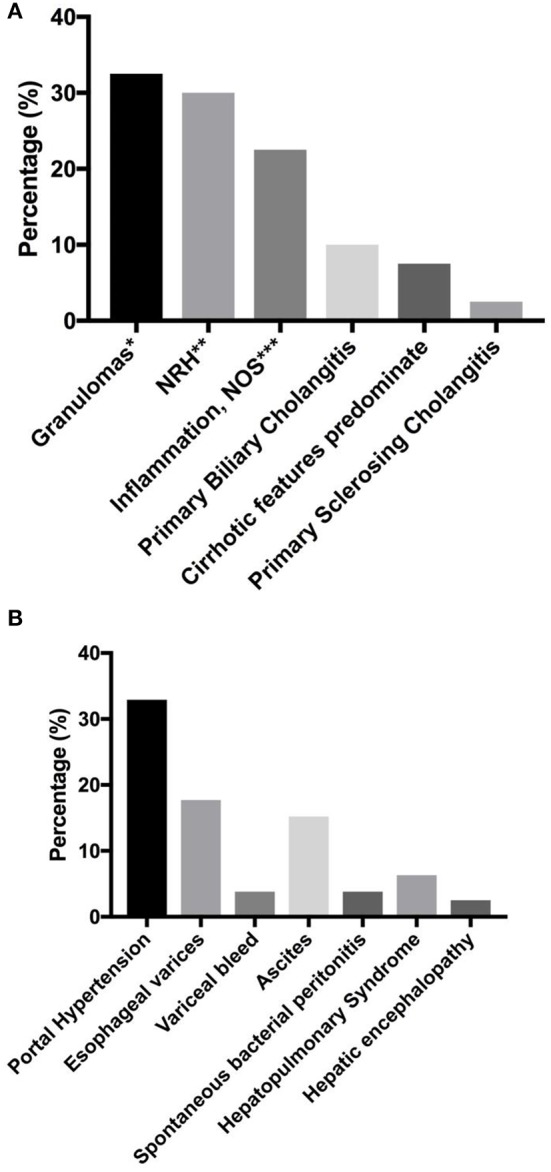
Non-infectious complications in common variable immunodeficiency (CVID) have emerged as a major clinical challenge. Detailed clinical spectrum, organ-specific pathologies and associated sequelae from 623 CVID patients followed in New York since 1974 were analyzed, and recent insights to pathogenesis were reviewed. Non-infectious manifestations were present in 68.1% of patients, and they do not tend to be present in isolation. They include autoimmunity (33.2%), chronic lung disease (30.3%), lymphoid hyperplasia/splenomegaly (20.9%), liver disease (12.7%), granulomas (9.3%), gastrointestinal disease (7.3%), lymphoma (6.7%), and other malignancies (6.4%). In the lungs, interstitial disease and bronchiectasis were the most common findings, with lymphoma at this site being a rare ( = 6), but serious, manifestation. Bronchiectasis was not a prerequisite for the development of interstitial disease. In the liver, granulomas and nodular regenerative hyperplasia were the most common. Gastrointestinal disease may affect any segment of the intestinal tract, with lymphoid infiltrations and villous blunting being the leading histologic findings. With progression of organ-specific diseases, a wide spectrum of associated sequelae was observed. Lymphoma was more common in females ( = 0.036)-all B cell types except in one subject. Solid organ transplantations (liver, = 5; lung, = 4; combined lung and heart, = 2) and hematopoietic stem cell transplantations (for B cell lymphoma, = 1) have rarely been performed in this cohort, with mixed outcomes. Recent identification of monogenic defects, in ~10-30% of various CVID cohorts, has highlighted the molecular pathways that can affect both antibody production and broader immune regulation. In addition, cellular defects in both innate and adaptive immune systems are increasingly recognized in this syndrome.
常见变异性免疫缺陷病(CVID)中的非感染性并发症已成为主要的临床挑战。分析了自 1974 年以来在纽约接受治疗的 623 例 CVID 患者的详细临床谱、器官特异性病理学和相关后遗症,并回顾了最近对发病机制的认识。68.1%的患者存在非感染性表现,而且这些表现并非孤立存在。它们包括自身免疫(33.2%)、慢性肺部疾病(30.3%)、淋巴组织增生/脾肿大(20.9%)、肝脏疾病(12.7%)、肉芽肿(9.3%)、胃肠道疾病(7.3%)、淋巴瘤(6.7%)和其他恶性肿瘤(6.4%)。在肺部,间质性疾病和支气管扩张症最为常见,而该部位的淋巴瘤则是一种罕见(=6)但严重的表现。支气管扩张症不是间质性疾病发展的必要条件。在肝脏,肉芽肿和结节性再生性增生最为常见。胃肠道疾病可能影响肠道的任何部位,以淋巴浸润和绒毛变钝为主要组织学表现。随着特定器官疾病的进展,观察到广泛的相关后遗症。女性中淋巴瘤更为常见(=0.036)-除了一个病例外,均为 B 细胞类型。该队列中很少进行实体器官移植(肝脏,=5;肺,=4;肺和心脏联合移植,=2)和造血干细胞移植(用于 B 细胞淋巴瘤,=1),结果不一。最近在各种 CVID 队列中约 10-30%的单基因缺陷的鉴定突显了可影响抗体产生和更广泛免疫调节的分子途径。此外,在该综合征中越来越多地认识到固有和适应性免疫系统的细胞缺陷。