Agha Ali M, Gill Clarence, Balanescu Dinu Valentin, Donisan Teodora, Palaskas Nicolas, Lopez-Mattei Juan, Hassan Saamir, Kim Peter Y, Charitakis Konstantinos, Cilingiroglu Mehmet, Oo Thein Hlaing, Kroll Michael, Durand Jean Bernard, Hirsch-Ginsberg Cheryl, Marmagkiolis Konstantinos, Iliescu Cezar
Department of Internal Medicine, University of Texas Health Science Center at Houston, Houston, TX, United States.
Department of Cardiology, University of Texas Health Science Center at Houston, Houston, TX, United States.
Front Cardiovasc Med. 2020 Feb 14;7:9. doi: 10.3389/fcvm.2020.00009. eCollection 2020.
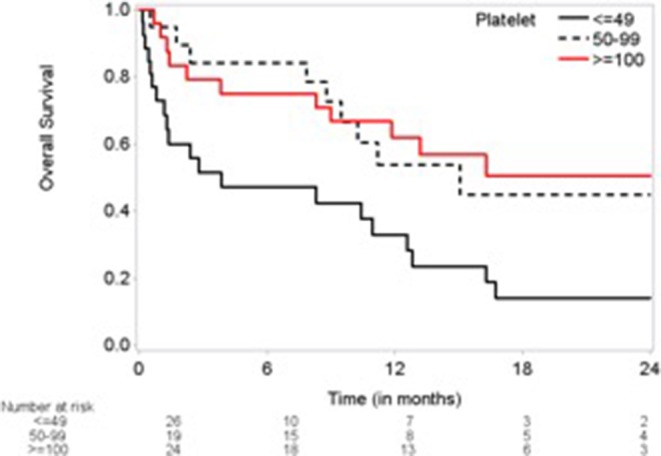
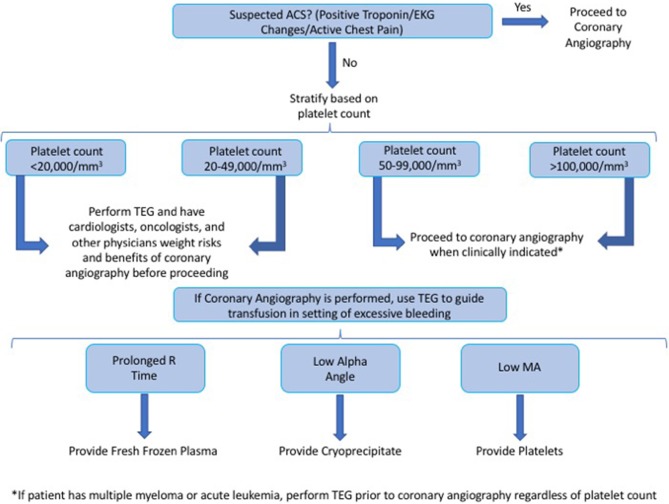
To evaluate the role of platelet count and thromboelastogram (TEG) in the treatment of thrombocytopenic cancer patients with suspected coronary artery disease (CAD). Cancer patients with CAD and thrombocytopenia are often treated non-invasively (i.e., without coronary angiography when clinically indicated) due to perceived high risk of bleeding. We sought to evaluate coagulability based on TEG and determine if platelet count and TEG could predict bleeding risk/mortality among cancer patients undergoing coronary angiography (CA). Baseline demographics, platelet count, and TEG parameters were recorded among cancer patients that underwent CA and had a concomitant TEG. Logistic regression and univariate proportional hazards regression analysis were performed to determine the impact of platelet count and coagulability on 24-month overall survival (OS). All patients with platelet count <20,000/mm and nearly all patients with platelet count 20,000-49,000/mm were hypocoagulable based on TEG results. In contrast, nearly all patients with platelet counts of 50,000-99,999/mm had normal TEG results and OS similar to those with platelet counts of ≥100,000/mm. Coagulability based on TEG was not associated with OS. However, a platelet count of <50,000/mm was associated with worse 24-month OS (hazard ratio = 2.76; = 0.0072) when compared with a platelet count of ≥100,000/mm. No major bleeding complications were observed in all groups. The majority of cancer patients with platelet counts of <50,000/mm were hypocoagulable based on TEG and had worse OS at 24 months. The relatively normal TEGs in the >50,000/mm groups, as well as the improved survival, suggest that with appropriate clinical indication and risk/benefit assessment, a cut-off of 50,000/mm platelets can be considered for CA in cancer patients.
评估血小板计数和血栓弹力图(TEG)在疑似冠状动脉疾病(CAD)的血小板减少症癌症患者治疗中的作用。患有CAD和血小板减少症的癌症患者由于被认为出血风险高,通常采用非侵入性治疗(即临床指征明确时不进行冠状动脉造影)。我们试图基于TEG评估凝血能力,并确定血小板计数和TEG是否可以预测接受冠状动脉造影(CA)的癌症患者的出血风险/死亡率。记录接受CA并同时进行TEG检测的癌症患者的基线人口统计学数据、血小板计数和TEG参数。进行逻辑回归和单变量比例风险回归分析,以确定血小板计数和凝血能力对24个月总生存期(OS)的影响。根据TEG结果,所有血小板计数<20,000/mm的患者以及几乎所有血小板计数为20,000 - 49,000/mm的患者均为低凝状态。相比之下,几乎所有血小板计数为50,000 - 99,999/mm的患者TEG结果正常,OS与血小板计数≥100,000/mm的患者相似。基于TEG的凝血能力与OS无关。然而,与血小板计数≥100,000/mm相比,血小板计数<50,000/mm与24个月时较差的OS相关(风险比 = 2.76; = 0.0072)。所有组均未观察到重大出血并发症。大多数血小板计数<50,000/mm的癌症患者基于TEG为低凝状态,且24个月时OS较差。血小板计数>50,000/mm组相对正常的TEG以及生存率的提高表明,在有适当的临床指征和风险/效益评估的情况下,癌症患者进行CA时可考虑将血小板计数临界值设定为50,000/mm。