Kersey Cooper B, Flaherty Kathleen R, Goldenthal Isaac L, Bokhari Sabahat, Biviano Angelo B
University of Washington School of Medicine, Department of Medicine, 1959 NE Pacific St, Seattle, WA 98195, USA.
Division of Cardiology, Internal Medicine, Irving Medical Center, Columbia University, 622 W 168th St, New York, NY 10032, USA.
Eur Heart J Case Rep. 2019 Oct 30;3(4):1-7. doi: 10.1093/ehjcr/ytz188. eCollection 2019 Dec.
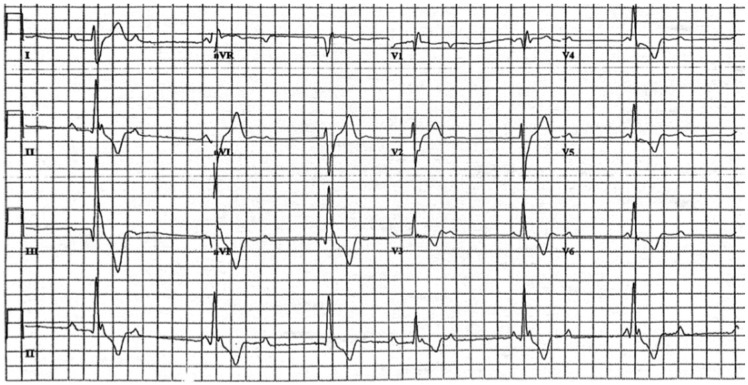
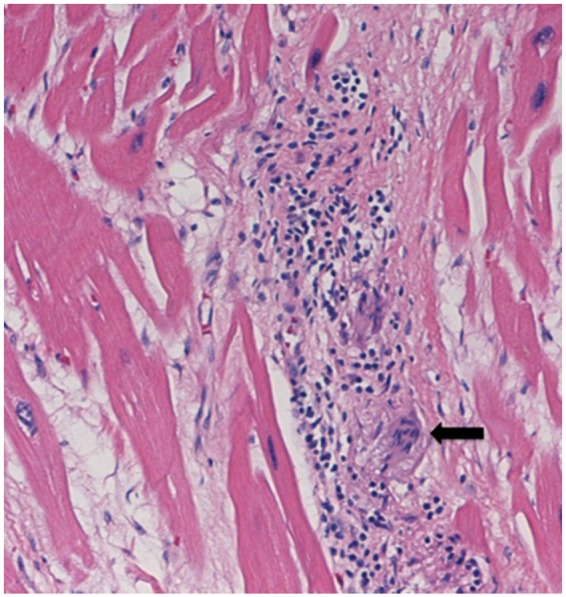
Clinically evident cardiac involvement has been documented in 5% of sarcoidosis patients, primarily manifesting as heart block, ventricular arrhythmias, and heart failure. Heart Rhythm Society consensus guidelines recommend advanced cardiac imaging with fluorodeoxyglucose-positron emission tomography (FDG-PET) scan for diagnosis of cardiac sarcoidosis, given endomyocardial biopsy's low sensitivity.
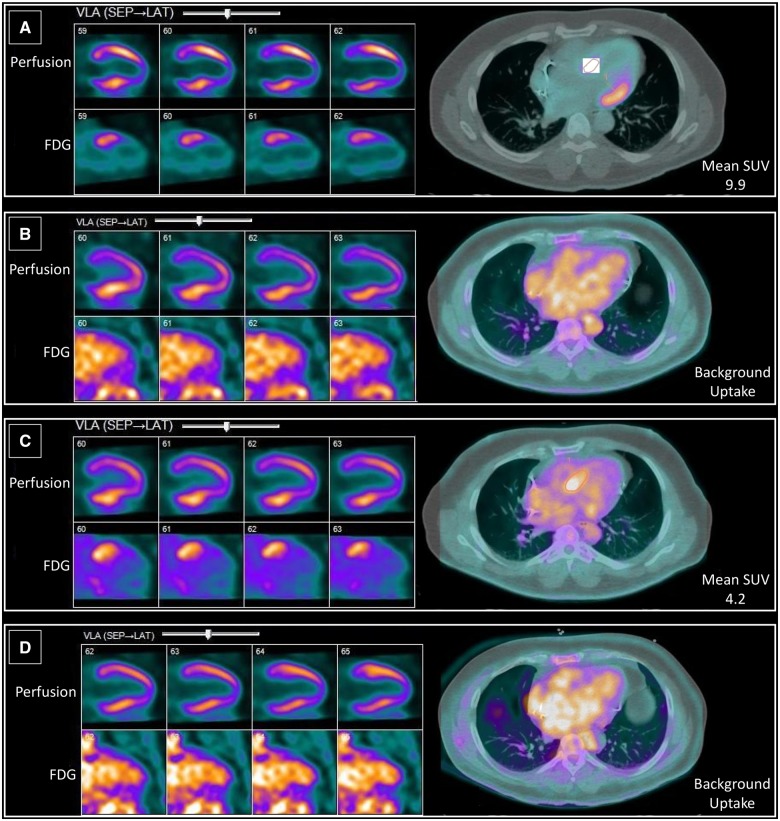
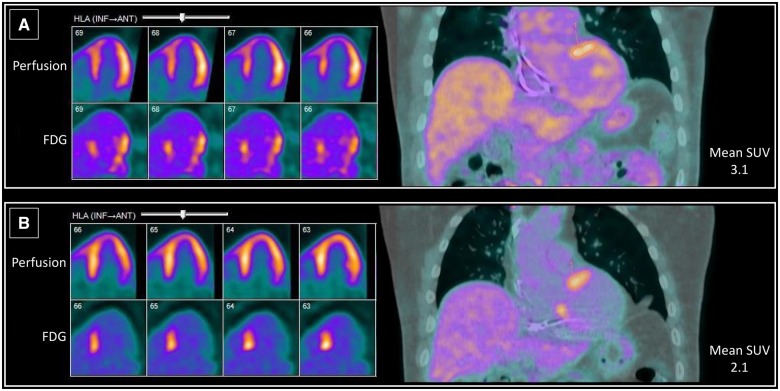
We describe four patients with cardiac sarcoidosis diagnosed with FDG-PET scan performed using a standardized imaging protocol for cardiac sarcoidosis. Serial FDG-PET scans were performed to monitor disease progression and response to therapy. Patients 1 and 2 presented with heart block, Patient 3 with heart failure and ventricular tachycardia (VT), and Patient 4 with VT. Patient 1 showed an initial decrease in standard uptake value (SUV) on immunosuppression, followed by an increase in SUV, necessitating steroid therapy. Patient 2's SUV decreased on immunosuppression. Patient 3 required 3.5 years of immunosuppression for the SUV to decrease to inactive disease levels, with SUV increasing and decreasing at different times during treatment, and subsequently developed VT. For Patient 4, areas of inflammation on the initial scan matched low voltage areas on the patient's EP study, confirming the arrhythmia's pathophysiological basis.
Cardiac sarcoidosis progression and response to therapy are heterogeneous. Serial FDG-PET scans are useful to diagnose disease, tailor therapy, and monitor the clinical course of disease, allowing treatment decisions to be based on the quantitative level of inflammation seen on FDG-PET.
据记载,5%的结节病患者有明显的心脏受累,主要表现为心脏传导阻滞、室性心律失常和心力衰竭。鉴于心内膜活检的敏感性较低,心律协会共识指南推荐使用氟脱氧葡萄糖-正电子发射断层扫描(FDG-PET)进行高级心脏成像以诊断心脏结节病。
我们描述了4例经FDG-PET扫描诊断为心脏结节病的患者,该扫描采用了标准化的心脏结节病成像方案。进行了系列FDG-PET扫描以监测疾病进展和对治疗的反应。患者1和患者2表现为心脏传导阻滞,患者3表现为心力衰竭和室性心动过速(VT),患者4表现为VT。患者1在免疫抑制治疗初期标准摄取值(SUV)下降,随后SUV升高,因此需要使用类固醇治疗。患者2的SUV在免疫抑制治疗期间下降。患者3需要3.5年的免疫抑制治疗,SUV才降至疾病非活动水平,治疗期间SUV在不同时间有升有降,随后发生了VT。对于患者4,初始扫描时的炎症区域与患者心内电生理检查中的低电压区域相匹配,证实了心律失常的病理生理基础。
心脏结节病的进展和对治疗的反应具有异质性。系列FDG-PET扫描有助于疾病诊断、调整治疗方案以及监测疾病的临床进程,使治疗决策能够基于FDG-PET上所见炎症的定量水平。