Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, South Carolina.
Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, Maryland.
Prostate. 2020 May;80(6):527-544. doi: 10.1002/pros.23967. Epub 2020 Mar 4.
For specific clinical indications, androgen deprivation therapy (ADT) will induce disease prostate cancer (PC) regression, relieve symptoms and prolong survival; however, ADT has a well-described range of side effects, which may have a detrimental effect on the patient's quality of life, necessitating additional interventions or changes in PC treatment. The risk-benefit analysis for initiating ADT in PC patients throughout the PC disease continuum warrants review.
A 14-member panel comprised of urologic and medical oncologists were chosen for an expert review panel, to provide guidance on a more judicious use of ADT in advanced PC patients. Panel members were chosen based upon their academic and community experience and expertise in the management of PC patients. Four academic members of the panel served as group leaders; the remaining eight panel members were from Large Urology Group Practice Association practices with proven experience in leading their advanced PC clinics. The panel members were assigned to four separate working groups, and were tasked with addressing the role of ADT in specific PC settings.
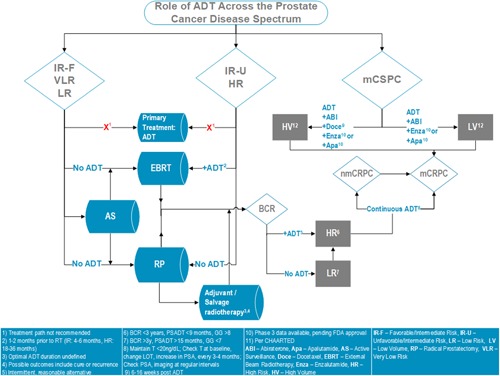
This article describes the practical recommendations of an expert panel for the use of ADT throughout the PC disease continuum, as well as an algorithm summarizing the key recommendations. The target for this publication is all providers (urologists, medical oncologists, radiation oncologists, or advanced practice providers) who evaluate and manage advanced PC patients, regardless of their practice setting.
The panel has provided recommendations for monitoring PC patients while on ADT, recognizing that PC patients will progress despite testosterone suppression and, therefore, early identification of conversion from castrate-sensitive to castration resistance is critical. Also, the requirement to both identify and mitigate side effects of ADT as well as the importance of quality of life maintenance are essential to the optimization of patient care, especially as more combinatorial therapeutic strategies with ADT continue to emerge.
对于特定的临床指征,雄激素剥夺疗法(ADT)会诱导前列腺癌(PC)消退,缓解症状并延长生存时间;然而,ADT 具有一系列明确的副作用,这可能对患者的生活质量产生不利影响,需要对 PC 治疗进行额外的干预或改变。需要对整个 PC 疾病进程中开始 ADT 的风险效益进行分析。
选择了 14 名泌尿科医生和肿瘤内科医生组成专家审查小组,为晚期 PC 患者更明智地使用 ADT 提供指导。小组成员根据他们在管理 PC 患者方面的学术和社区经验以及专业知识进行选择。小组中有 4 名学术成员担任组长,其余 8 名成员来自大型泌尿科集团实践协会,在领导其晚期 PC 诊所方面具有丰富的经验。小组成员被分配到四个独立的工作组,负责解决 ADT 在特定 PC 环境中的作用。
本文描述了一个专家小组在整个 PC 疾病进程中使用 ADT 的实用建议,以及总结关键建议的算法。本文的目标读者是所有评估和管理晚期 PC 患者的提供者(泌尿科医生、肿瘤内科医生、放射肿瘤学家或高级实践提供者),无论其实践环境如何。
该小组为接受 ADT 治疗的 PC 患者提供了监测建议,认识到尽管睾酮被抑制,但 PC 患者仍会进展,因此,早期识别从去势敏感型到去势抵抗型的转变至关重要。此外,识别和减轻 ADT 的副作用以及维持生活质量的重要性是优化患者护理的关键,特别是随着越来越多的与 ADT 相结合的治疗策略不断涌现。