Sharma Sonia G, Levine Steven N, Yatavelli Rajini K, Shaha Manish A, Nathan Cherie Ann O
Department of Medicine, Division of Endocrinology, Diabetes and Metabolism, Louisiana State University Health Sciences Center, Shreveport, Louisiana.
Department of Otolaryngology-Head and Neck Surgery, Louisiana State University Health Sciences Center, Shreveport, Louisiana.
J Endocr Soc. 2020 Feb 5;4(3):bvaa015. doi: 10.1210/jendso/bvaa015. eCollection 2020 Mar 1.
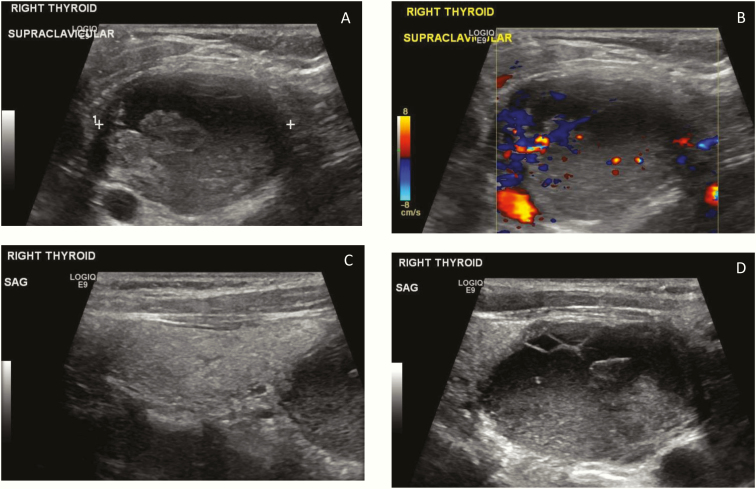
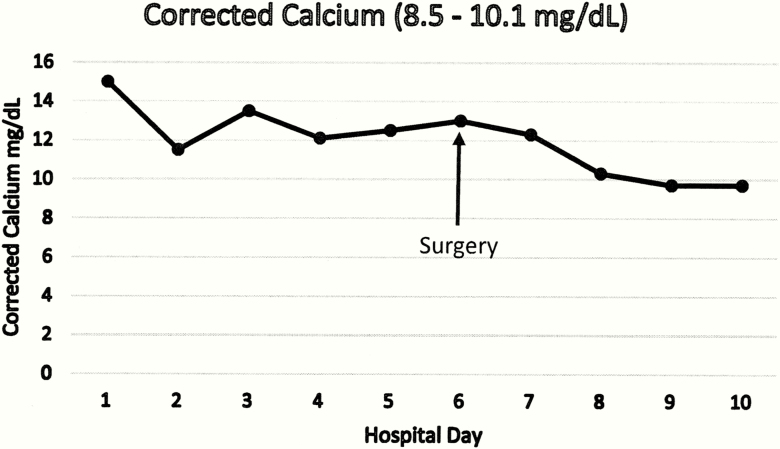
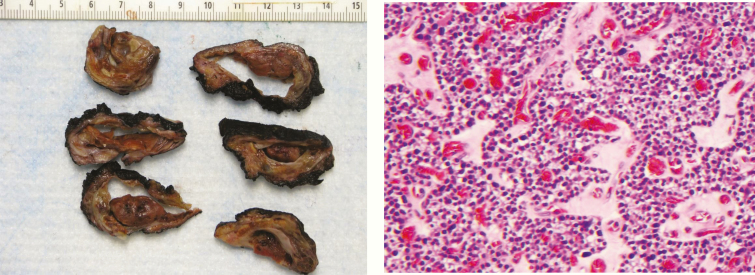
Primary hyperparathyroidism is not commonly diagnosed during pregnancy. For pregnant women with mild, asymptomatic disease, surgery can be avoided unless the degree of hypercalcemia becomes more severe or they develop complications. However, there are no evidence-based guidelines to assist clinicians regarding the management of primary hyperparathyroidism during pregnancy. When surgery is deemed necessary during pregnancy, the second trimester is generally considered to be the optimal time. We report the case of a 31-year-old female G1P0 who presented at 6 weeks gestation with symptoms of nausea, vomiting, polyuria, and corrected calcium of 14.8 mg/dL. Due to the extreme degree of hypercalcemia and refractory to medical treatment, it was decided that surgery could not be delayed until the second trimester. At 7w3d gestational age the patient had resection of a 37 gram, 5 × 4 × 3 cm right inferior parathyroid adenoma.
原发性甲状旁腺功能亢进症在孕期并不常见。对于患有轻度无症状疾病的孕妇,除非高钙血症程度加重或出现并发症,否则可避免手术。然而,目前尚无循证指南可协助临床医生处理孕期原发性甲状旁腺功能亢进症。当孕期认为有必要进行手术时,孕中期通常被视为最佳时机。我们报告一例31岁初孕女性,孕6周时出现恶心、呕吐、多尿症状,校正血钙为14.8mg/dL。由于高钙血症程度极重且药物治疗无效,决定手术不能推迟至孕中期。孕7周3天时,患者切除了一个重37克、大小为5×4×3厘米的右下甲状旁腺腺瘤。