Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
Now with the Feinberg School of Medicine, Division of Biostatistics, Department of Preventive Medicine, Northwestern University, Chicago, Illinois.
JAMA Netw Open. 2020 Mar 2;3(3):e200452. doi: 10.1001/jamanetworkopen.2020.0452.
The Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database may provide insights into the comparative effectiveness of oncological treatments for elderly individuals who are underrepresented in clinical trials.
To evaluate the suitability of SEER-Medicare data for assessing the effectiveness of adding a drug to an existing treatment regimen on the overall survival of elderly patients with cancer.
DESIGN, SETTING, AND PARTICIPANTS: This comparative effectiveness study analyzed SEER-Medicare data from 9549 individuals who received a new diagnosis of stage II colorectal cancer (2008-2012) and 940 patients who received a new diagnosis of advanced pancreatic adenocarcinoma (2007-2012), with follow-up to December 31, 2013 (SEER-Medicare data released in 2015). Two (hypothetical) target trials were designed and emulated based on 2 existing randomized clinical trials: (1) adjuvant fluorouracil after curative surgery for individuals with stage II colorectal cancer and (2) erlotinib added to gemcitabine for individuals with advanced pancreatic adenocarcinoma. Data were analyzed January 2018 to March 2019.
The following treatment strategies were compared: (1) fluorouracil initiation vs no initiation within 3 months of tumor resection and (2) erlotinib initiation vs no initiation within 12 weeks of gemcitabine initiation.
All-cause mortality within 60 months of baseline for the fluorouracil trial and within 72 weeks for the erlotinib trial.
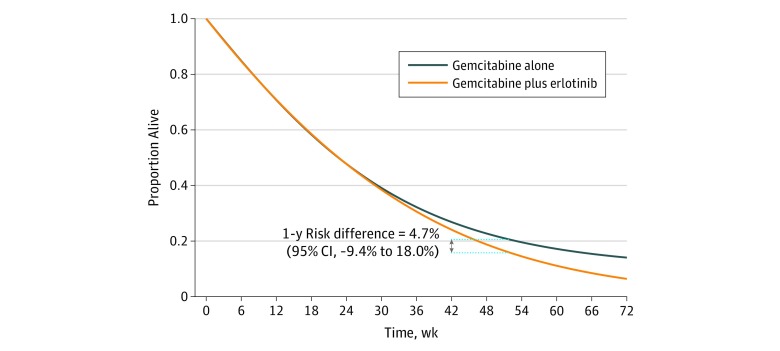
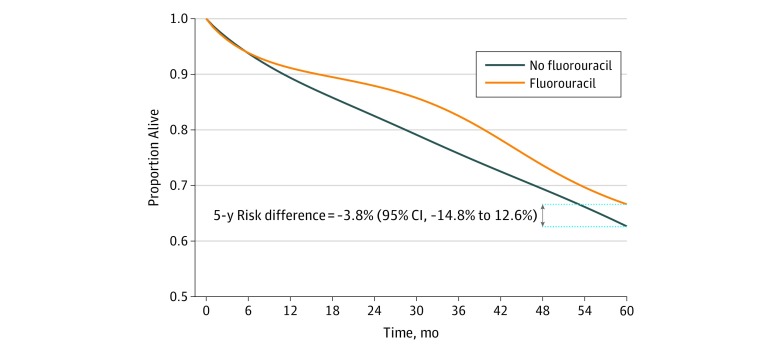
Compared with 3293 individuals in the existing fluorouracil trial, 9549 eligible individuals included in the present analyses were more likely to have colon cancer (8565 [90%] vs 2291 [71%]) and were older (median [interquartile range], 79 [73-84] vs 63 [56-68] years). The 5-year risk difference for initiation vs noninitiation of fluorouracil after surgery was -3.8% (95% CI, -14.8% to 12.6%), and the mortality hazard ratio (HR) was 0.95 (95% CI, 0.85-1.04). Compared with 569 individuals in the existing erlotinib trial, 940 eligible patients included in the present analysis were older (median [range], 74 [66-93] vs 64 [36-92] years) and more likely to be male (547 [58%] vs 298 [52%]). The 1-year risk difference for initiation vs noninitiation of erlotinib was 4.7% (95% CI, -9.4% to 18.0%), and the corresponding mortality HR was 1.04 (95% CI, 0.86-1.42). In naive analyses, the mortality HR estimate was 1.14 (95% CI, 0.95-1.36) for the fluorouracil emulation and 0.68 (95% CI, 0.54-0.87) for the erlotinib emulation.
The present estimates were similar to those from randomized clinical trials that studied adding the same cancer drugs to existing regimens. The published HR was 1.02 (95% CI, 0.70-1.48) in the fluorouracil trial for individuals aged 70 or older and 0.96 (95% CI, 0.74-1.24) in the erlotinib trial for individuals aged 65 years or older. The SEER-Medicare database may be adequate for studying the real-world effectiveness of adding a drug to treatment regimens used for elderly individuals with cancer.
监测、流行病学和最终结果(SEER)-医疗保险数据库可能为了解临床试验中代表性不足的老年患者的肿瘤治疗的比较效果提供线索。
评估 SEER-医疗保险数据在评估将药物添加到现有治疗方案中对患有癌症的老年患者的总生存期的有效性方面的适用性。
设计、设置和参与者:这项比较有效性研究分析了来自 9549 名接受 II 期结直肠癌新诊断(2008-2012 年)和 940 名接受晚期胰腺腺癌新诊断(2007-2012 年)的患者的 SEER-医疗保险数据,随访至 2013 年 12 月 31 日(2015 年发布的 SEER-医疗保险数据)。根据 2 项现有的随机临床试验设计了并模拟了两个(假设)目标试验:(1)II 期结直肠癌患者手术后辅助氟尿嘧啶治疗,(2)晚期胰腺腺癌患者加用厄洛替尼治疗吉西他滨。数据于 2018 年 1 月至 2019 年 3 月进行分析。
比较了以下治疗策略:(1)肿瘤切除后 3 个月内开始氟尿嘧啶治疗与不开始治疗,(2)吉西他滨治疗开始后 12 周内开始厄洛替尼治疗与不开始治疗。
氟尿嘧啶试验的 60 个月内和厄洛替尼试验的 72 周内的全因死亡率。
与现有氟尿嘧啶试验中的 3293 名患者相比,本分析中纳入的 9549 名合格患者更有可能患有结肠癌(8565[90%]与 2291[71%])且年龄更大(中位数[四分位距],79[73-84]与 63[56-68]岁)。手术后开始与不开始氟尿嘧啶治疗的 5 年风险差异为-3.8%(95%CI,-14.8%至 12.6%),死亡率的危险比(HR)为 0.95(95%CI,0.85-1.04)。与现有厄洛替尼试验中的 569 名患者相比,本分析中纳入的 940 名合格患者年龄更大(中位数[范围],74[66-93]与 64[36-92]岁)且更可能为男性(547[58%]与 298[52%])。开始与不开始厄洛替尼治疗的 1 年风险差异为 4.7%(95%CI,-9.4%至 18.0%),相应的死亡率 HR 为 1.04(95%CI,0.86-1.42)。在原始分析中,氟尿嘧啶模拟的死亡率 HR 估计值为 1.14(95%CI,0.95-1.36),厄洛替尼模拟的死亡率 HR 估计值为 0.68(95%CI,0.54-0.87)。
本研究结果与研究将相同癌症药物添加到现有方案中的随机临床试验结果相似。氟尿嘧啶试验中年龄在 70 岁或以上的患者的公布 HR 为 1.02(95%CI,0.70-1.48),厄洛替尼试验中年龄在 65 岁或以上的患者的公布 HR 为 0.96(95%CI,0.74-1.24)。SEER-医疗保险数据库可能足以研究将药物添加到用于治疗老年癌症患者的治疗方案中的实际效果。