Department of Emergency Medicine, University of Michigan, Ann Arbor.
Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor.
JAMA Netw Open. 2020 Mar 2;3(3):e200612. doi: 10.1001/jamanetworkopen.2020.0612.
Appendicitis may be missed during initial emergency department (ED) presentation.
To compare patients with a potentially missed diagnosis of appendicitis (ie, patients with symptoms associated with appendicitis, including abdominal pain, constipation, nausea and/or vomiting, fever, and diarrhea diagnosed within 1-30 days after initial ED presentation) with patients diagnosed with appendicitis on the same day of ED presentation to identify factors associated with potentially missed appendicitis.
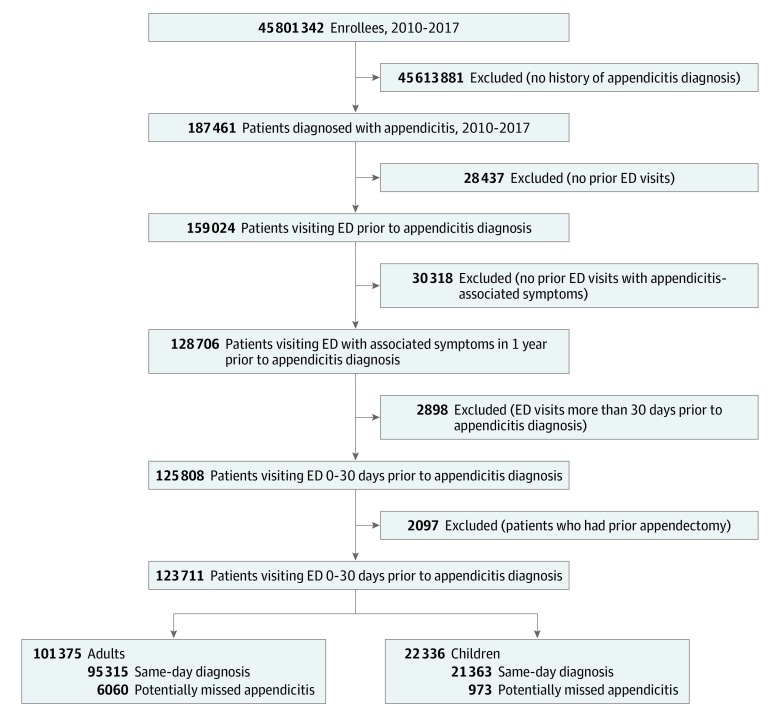
DESIGN, SETTING, AND PARTICIPANTS: In this cohort study, a retrospective analysis of commercially insured claims data was conducted from January 1 to December 15, 2019. Patients who presented to the ED with undifferentiated symptoms associated with appendicitis between January 1, 2010, and December 31, 2017, were identified using the Clinformatics Data Mart administrative database (Optum Insights). The study sample comprised eligible adults (aged ≥18 years) and children (aged <18 years) who had previous ED visits within 30 days of an appendicitis diagnosis.
Potentially missed diagnosis of appendicitis. Adjusted odds ratios (AORs) for abdominal pain and its combinations with other symptoms associated with appendicitis were compared between patients with a same-day diagnosis of appendicitis and patients with a potentially missed diagnosis of appendicitis.
Of 187 461 patients with a diagnosis of appendicitis, a total of 123 711 (66%; 101 375 adults [81.9%] and 22 336 children [18.1%]) were eligible for analysis. Among adults, 51 923 (51.2%) were women, with a mean (SD) age of 44.3 (18.2) years; among children, 9631 (43.1%) were girls, with a mean (SD) age of 12.2 (18.2) years. The frequency of potentially missed appendicitis was 6060 of 101 375 adults (6.0%) and 973 of 22 336 children (4.4%). Patients with isolated abdominal pain (adults, AOR, 0.65; 95% CI, 0.62-0.69; P < .001; children, AOR, 0.79; 95% CI, 0.69-0.90; P < .001) or with abdominal pain and nausea and/or vomiting (adults, AOR, 0.90; 95% CI, 0.84-0.97; P = .003; children, AOR, 0.84; 95% CI, 0.71-0.98; P = .03) were less likely to have missed appendicitis. Patients with abdominal pain and constipation (adults, AOR, 1.51; 95% CI, 1.31-1.75; P < .001; children, AOR, 2.43; 95% CI, 1.86-3.17; P < .001) were more likely to have missed appendicitis. Stratified by the presence of undifferentiated symptoms, women (abdominal pain, AOR, 1.68; 95% CI, 1.58-1.78; nausea and/or vomiting, AOR, 1.68; 95% CI, 1.52-1.85; fever, AOR, 1.32; 95% CI, 1.10-1.59; diarrhea, AOR, 1.19; 95% CI, 1.01-1.40; and constipation, AOR, 1.50; 95% CI, 1.24-1.82) and girls (abdominal pain, AOR, 1.64; 95% CI, 1.43-1.88; nausea and/or vomiting, AOR, 1.74; 95% CI, 1.42-2.13; fever, AOR, 1.55; 95% CI, 1.14-2.11; diarrhea, AOR, 1.80; 95% CI, 1.19-2.74; and constipation, AOR, 1.25; 95% CI, 0.88-1.78) as well as patients with a comorbidity index of 2 or greater (adults, abdominal pain, AOR, 3.33; 95% CI, 3.09-3.60; nausea and/or vomiting, AOR, 3.66; 95% CI, 3.23-4.14; fever, AOR, 5.00; 95% CI, 3.79-6.60; diarrhea, AOR, 4.27; 95% CI, 3.39-5.38; and constipation, AOR, 4.17; 95% CI, 3.08-5.65; children, abdominal pain, AOR, 2.42; 95% CI, 1.93-3.05; nausea and/or vomiting, AOR, 2.55; 95% CI, 1.89-3.45; fever, AOR, 4.12; 95% CI, 2.71-6.25; diarrhea, AOR, 2.17; 95% CI, 1.18-3.97; and constipation, AOR, 2.19; 95% CI, 1.30-3.70) were more likely to have missed appendicitis. Adult patients who received computed tomographic scans at the initial ED visit (abdominal pain, AOR, 0.58; 95% CI, 0.52-0.65; nausea and/or vomiting, AOR, 0.63; 95% CI, 0.52-0.75; fever, AOR, 0.41; 95% CI, 0.29-0.58; diarrhea, AOR, 0.83; 95% CI, 0.58-1.20; and constipation, AOR, 0.60; 95% CI, 0.39-0.94) were less likely to have missed appendicitis.
Regardless of age, a missed diagnosis of appendicitis was more likely to occur in women, patients with comorbidities, and patients who experienced abdominal pain accompanied by constipation. Population-based estimates of the rates of potentially missed appendicitis reveal opportunities for improvement and identify factors that may mitigate the risk of a missed diagnosis.
重要性:在初始急诊就诊时,阑尾炎可能会被漏诊。
目的:比较潜在漏诊阑尾炎(即有阑尾炎相关症状的患者,包括腹痛、便秘、恶心和/或呕吐、发热和腹泻,这些症状在急诊就诊后 1-30 天内被诊断)与在同一天因腹痛就诊的阑尾炎患者,以确定潜在漏诊阑尾炎相关的因素。
设计、地点和参与者:在这项基于队列的研究中,回顾性分析了 2019 年 1 月 1 日至 12 月 15 日期间商业保险索赔数据的临床信息数据集市。使用 Optum Insights 中的 Clinformatics Data Mart 行政数据库,从 2010 年 1 月 1 日至 2017 年 12 月 31 日期间,确定了有未分化症状与阑尾炎相关且在阑尾诊断前 30 天内有先前急诊就诊的符合条件的成年人(年龄≥18 岁)和儿童(年龄<18 岁)。
主要结果和措施:潜在的阑尾炎漏诊。对同一天诊断为阑尾炎和潜在漏诊阑尾炎的患者的腹痛及其与阑尾炎相关的其他症状的组合进行调整后的优势比(AOR)比较。
结果:在 187461 例阑尾炎诊断患者中,共有 123711 例(66%;101375 例成年人[81.9%]和 22336 例儿童[18.1%])符合分析条件。在成年人中,51923 例(51.2%)为女性,平均(SD)年龄为 44.3(18.2)岁;在儿童中,9631 例(43.1%)为女孩,平均(SD)年龄为 12.2(18.2)岁。潜在漏诊阑尾炎的频率为 101375 例成年人中的 6060 例(6.0%)和 22336 例儿童中的 973 例(4.4%)。仅腹痛(成年人,AOR,0.65;95%置信区间,0.62-0.69;P<0.001;儿童,AOR,0.79;95%置信区间,0.69-0.90;P<0.001)或腹痛伴恶心和/或呕吐(成年人,AOR,0.90;95%置信区间,0.84-0.97;P=0.003;儿童,AOR,0.84;95%置信区间,0.71-0.98;P=0.03)的患者不太可能漏诊阑尾炎。腹痛伴便秘(成年人,AOR,1.51;95%置信区间,1.31-1.75;P<0.001;儿童,AOR,2.43;95%置信区间,1.86-3.17;P<0.001)的患者更有可能漏诊阑尾炎。按未分化症状分层,女性(腹痛,AOR,1.68;95%置信区间,1.58-1.78;恶心和/或呕吐,AOR,1.68;95%置信区间,1.52-1.85;发热,AOR,1.32;95%置信区间,1.10-1.59;腹泻,AOR,1.19;95%置信区间,1.01-1.40;便秘,AOR,1.50;95%置信区间,1.24-1.82)和女孩(腹痛,AOR,1.64;95%置信区间,1.43-1.88;恶心和/或呕吐,AOR,1.74;95%置信区间,1.42-2.13;发热,AOR,1.55;95%置信区间,1.14-2.11;腹泻,AOR,1.80;95%置信区间,1.19-2.74;便秘,AOR,1.25;95%置信区间,0.88-1.78)以及合并症指数为 2 或更高的患者(成年人,腹痛,AOR,3.33;95%置信区间,3.09-3.60;恶心和/或呕吐,AOR,3.66;95%置信区间,3.23-4.14;发热,AOR,5.00;95%置信区间,3.79-6.60;腹泻,AOR,4.27;95%置信区间,3.39-5.38;便秘,AOR,4.17;95%置信区间,3.08-5.65;儿童,腹痛,AOR,2.42;95%置信区间,1.93-3.05;恶心和/或呕吐,AOR,2.55;95%置信区间,1.89-3.45;发热,AOR,4.12;95%置信区间,2.71-6.25;腹泻,AOR,2.17;95%置信区间,1.18-3.97;便秘,AOR,2.19;95%置信区间,1.30-3.70)更有可能漏诊阑尾炎。在初始急诊就诊时接受计算机断层扫描的成年患者(腹痛,AOR,0.58;95%置信区间,0.52-0.65;恶心和/或呕吐,AOR,0.63;95%置信区间,0.52-0.75;发热,AOR,0.41;95%置信区间,0.29-0.58;腹泻,AOR,0.83;95%置信区间,0.58-1.20;便秘,AOR,0.60;95%置信区间,0.39-0.94)不太可能漏诊阑尾炎。
结论和相关性:无论年龄大小,女性、合并症患者和出现腹痛伴便秘的患者更有可能出现阑尾炎漏诊。基于人群的潜在漏诊阑尾炎发生率的估计表明,存在改进的机会,并确定了可能降低漏诊风险的因素。