Research and Development Group, Center for Technology Innovation-Energy, Hitachi Ltd, Hitachi-shi, Ibaraki-ken, Japan.
Graduate School of Biomedical Science and Engineering, Hokkaido University, Sapporo, Hokkaido, Japan.
J Appl Clin Med Phys. 2020 Apr;21(4):42-50. doi: 10.1002/acm2.12844. Epub 2020 Mar 9.
While a large amount of experimental data suggest that the proton relative biological effectiveness (RBE) varies with both physical and biological parameters, current commercial treatment planning systems (TPS) use the constant RBE instead of variable RBE models, neglecting the dependence of RBE on the linear energy transfer (LET). To conduct as accurate a clinical evaluation as possible in this circumstance, it is desirable that the dosimetric parameters derived by TPS ( ) are close to the "true" values derived with the variable RBE models ( ). As such, in this study, the closeness of to was compared between planning target volume (PTV)-based and robust plans.
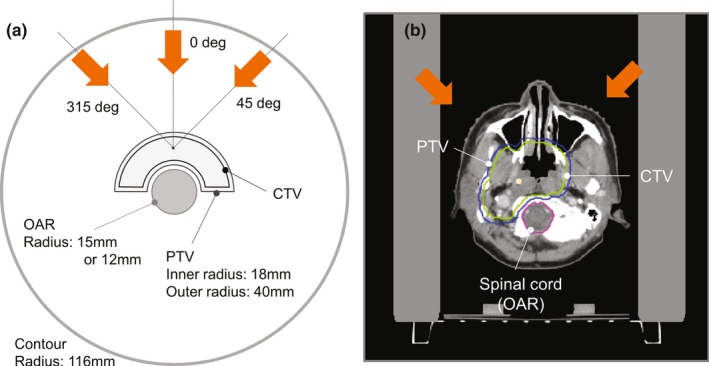
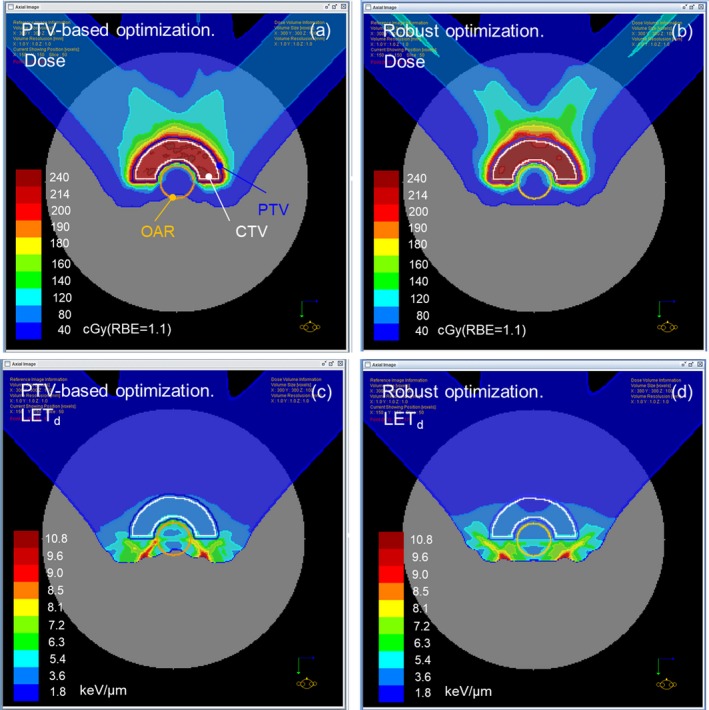
Intensity-modulated proton therapy (IMPT) treatment plans for two Radiation Therapy Oncology Group (RTOG) phantom cases and four nasopharyngeal cases were created using the PTV-based and robust optimizations, under the assumption of a constant RBE of 1.1. First, the physical dose and dose-averaged LET (LET ) distributions were obtained using the analytical calculation method, based on the pencil beam algorithm. Next, was calculated using three different RBE models. The deviation of from was evaluated with D and D , which have been used as the evaluation indices for clinical target volume (CTV) and organs at risk (OARs), respectively. The influence of the distance between the OAR and CTV on the results was also investigated. As a measure of distance, the closest distance and the overlapped volume histogram were used for the RTOG phantom and nasopharyngeal cases, respectively.
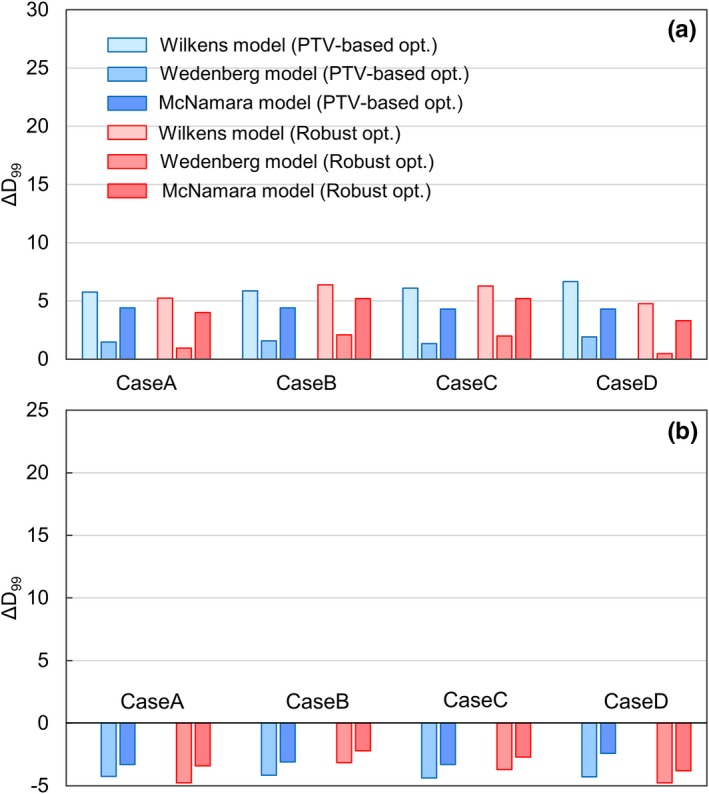
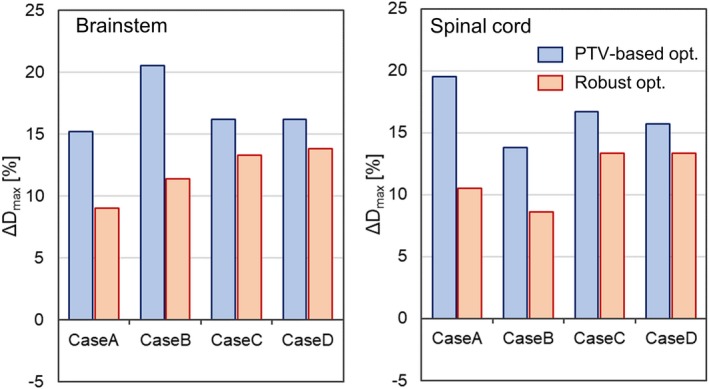
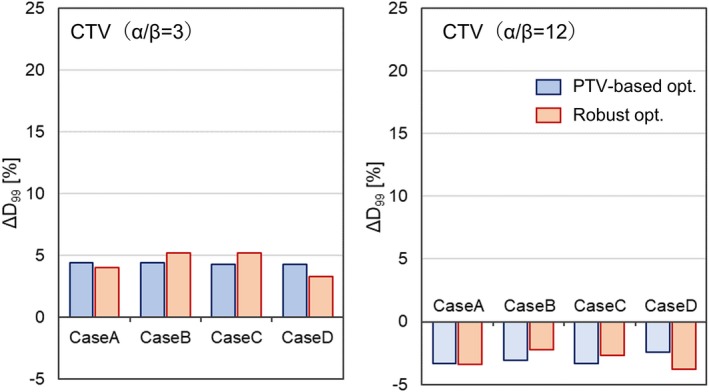
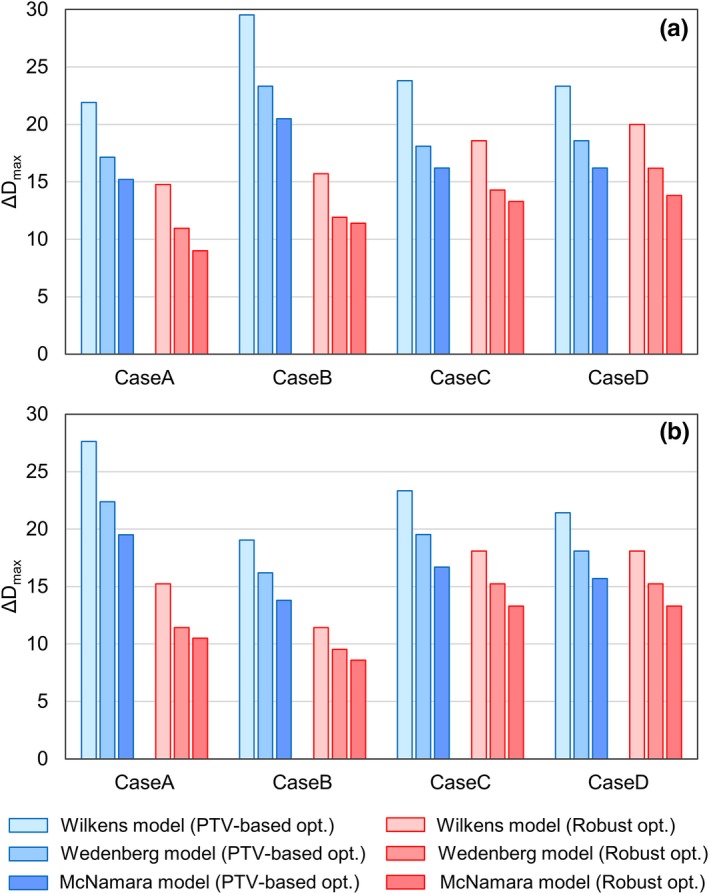
As for the OAR, the deviations of from were always smaller in robust plans than in PTV-based plans in all RBE models. The deviation would tend to increase as the OAR was located closer to the CTV in both optimization techniques. As for the CTV, the deviations of from were comparable between the two optimization techniques, regardless of the distance between the CTV and the OAR.
Robust optimization was found to be more favorable than PTV-based optimization in that the results presented by TPS were closer to the "true" values and that the clinical evaluation based on TPS was more reliable.
虽然大量实验数据表明质子相对生物学效应(RBE)随物理和生物学参数而变化,但目前的商业治疗计划系统(TPS)使用恒定 RBE 而不是可变 RBE 模型,忽略了 RBE 对线性能量转移(LET)的依赖性。在这种情况下,为了尽可能进行准确的临床评估,希望 TPS 得出的剂量学参数()尽可能接近使用可变 RBE 模型得出的“真实”值()。因此,在这项研究中,比较了基于计划靶区(PTV)和稳健计划的之间的接近程度。
在假设 RBE 为 1.1 的情况下,使用基于 PTV 和稳健优化的方法为两个放射治疗肿瘤学组(RTOG)体模病例和四个鼻咽癌病例创建强度调制质子治疗(IMPT)治疗计划。首先,使用基于笔形束算法的解析计算方法获得物理剂量和剂量平均 LET(LET)分布。接下来,使用三种不同的 RBE 模型计算。使用 D 和 D,评估与之间的偏差,D 和 D 分别是临床靶区(CTV)和危及器官(OAR)的评估指标。还研究了 OAR 和 CTV 之间距离对结果的影响。作为距离的度量,使用最近距离和重叠体积直方图分别用于 RTOG 体模和鼻咽癌病例。
对于 OAR,在所有 RBE 模型中,稳健计划中从到的偏差总是小于 PTV 基计划。在两种优化技术中,随着 OAR 更靠近 CTV,偏差趋于增加。对于 CTV,无论 CTV 和 OAR 之间的距离如何,两种优化技术之间的偏差都可以比较。
与 PTV 基优化相比,稳健优化更有利,因为 TPS 呈现的结果更接近“真实”值,并且基于 TPS 的临床评估更可靠。